The revenue cycle management market is growing fast, but the bigger story for providers is operational pressure. More organizations are investing in integrated RCM platforms because disconnected intake, billing, coding, and follow-up processes create delays, rework, and margin loss.
Best practice revenue cycle management works as an operating model. It ties front-end intake, coding, claims, denials, patient collections, payer contracts, analytics, and compliance into a process leaders can measure and improve. Without that structure, staff time shifts toward fixing avoidable errors instead of protecting cash flow.
In practice, the highest-impact improvements are rarely flashy. Registration controls reduce downstream edits. Coding feedback reduces preventable denials. Clear work queues improve follow-up on aging claims. Contract reviews catch underpayments that would otherwise pass unnoticed. Analytics help only when managers use them to make weekly operating decisions.
The playbook below is built for execution. Each best practice is broken into what it affects, how to put it in place, and the trade-offs teams should expect while they change the process.
Table of Contents
- 1. Front-End Revenue Cycle Optimization
- 2. Clean Claim Submission and Coding Accuracy Standards
- 3. Proactive Claims Follow-Up and Management System
- 4. Denial Management and Root Cause Analysis Program
- 5. Patient Financial Responsibility Management and Collections Strategy
- 6. Payer Contract Management and Fee Schedule Optimization
- 7. Revenue Cycle Technology Integration and Data Analytics
- 8. Compliance and Risk Management in Revenue Cycle Operations
- 8-Point Revenue Cycle Management Comparison
- From Best Practices to Better Performance
1. Front-End Revenue Cycle Optimization
Upstream errors are expensive. A wrong subscriber ID, missed authorization, or incomplete coordination of benefits at intake can turn a payable claim into avoidable rework, patient confusion, and delayed cash.
Front-end performance sets the operating ceiling for the rest of revenue cycle management. If registration accuracy is weak, clean claims, denial prevention, and patient collections all get harder. In practice, the highest-performing teams treat patient access as a control point, not a scheduling task.
The playbook starts before the patient arrives. Use pre-visit workflows to verify eligibility, confirm coverage order, identify authorization requirements, and estimate patient responsibility early enough for staff to fix exceptions before date of service. Integrated systems help because they keep verification, authorization status, scheduling notes, and downstream billing activity in one place. The primary advantage is not software consolidation by itself. It is fewer handoffs, clearer accountability, and less duplicated work across access, billing, and follow-up teams.

Verify before the visit, not after the denial
A front-end process that holds up under pressure usually includes four parts:
- Start eligibility checks before the appointment is finalized: Run electronic verification early enough to catch inactive coverage, plan changes, and demographic mismatches before the patient is in the office.
- Escalate high-risk encounters for manual review: Surgery, imaging, infusion, and other high-dollar services often need benefit review, prior authorization confirmation, or service-specific payer rules checked by a person.
- Build a true exception workflow: Unverified coverage, self-pay conversions, workers' compensation, and accident-related visits should move to a separate queue with ownership and turnaround targets.
- Use registration scripts that surface hidden problems: Staff should ask about secondary coverage, recent employer changes, referral requirements, and accident details instead of relying on the card alone.
Impact should be measured in operating terms, not just effort. Track eligibility hit rate, authorization obtained before service, registration error rate by registrar, point-of-service collections, and denials tied to front-end defects. Those measures show whether the process is preventing downstream loss or just creating more clicks.
One implementation detail matters more than many teams expect. Required fields must actually be required. If staff can bypass prompts during peak volume, the process will fail at the busiest and most expensive moments. I have seen organizations add real-time eligibility tools and still struggle because registrars could override warnings without review. The fix was straightforward: lock key fields, require reason codes for exceptions, and send a weekly error report by payer, location, and employee.
Patient estimates belong here too, but only if they are credible. A vague estimate creates conflict at the desk and weakens collections. A usable estimate reflects verified benefits, expected service mix, and known authorization status. Teams that want fewer billing complaints should also train access staff on common medical coding errors that start upstream, because the handoff between registration, charge capture, and coding often breaks earlier than leaders think.
Practical rule: If staff cannot explain coverage status, authorization status, and expected patient responsibility in plain language before service, the front end is still incomplete.
A strong front end is not about slowing intake down. It is about deciding where precision matters most, then designing the workflow so the highest-risk encounters get the most attention before they become avoidable AR.
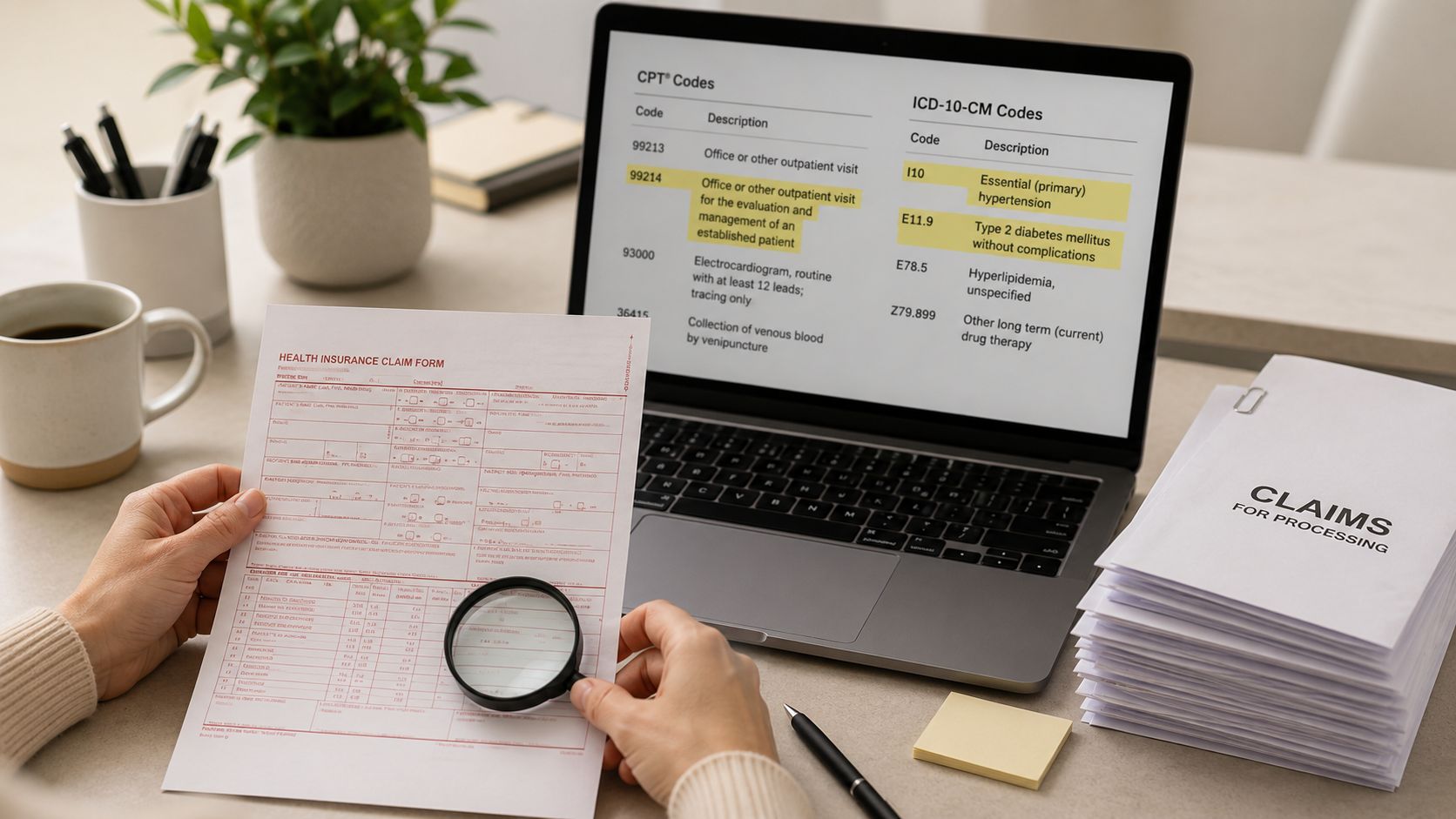
2. Clean Claim Submission and Coding Accuracy Standards
Coding errors remain one of the fastest ways to slow cash and create avoidable rework. Clean claims come from a controlled process that connects documentation, coding, charge capture, and claim edits before the bill ever reaches the payer.
A practical standard starts with timing. Charges need to post quickly enough that coders still have access to fresh documentation, clinicians can answer questions without delay, and billing staff can correct issues before filing deadlines tighten. In practice, that means setting a defined charge lag target, monitoring it by specialty, and reviewing any service line that regularly falls outside the standard.
A playbook for cleaner claims
Strong coding performance usually depends on four core requirements:
- Scrub claims before submission: Apply payer edits, NCCI logic, demographic validation, and modifier checks before claims leave the system.
- Review documentation and coding together: Code reviews without the clinical note miss the reason many claims fail medical necessity or diagnosis linkage checks.
- Give clinicians specific feedback: Point to the missing element, such as laterality, diagnosis-to-procedure support, time documentation, or operative detail.
- Track repeat error patterns by specialty and provider: Recurring mistakes usually signal a workflow or template problem, not just an individual training issue.
The impact is measurable. Better edit discipline reduces first-pass rejections. Better documentation review lowers preventable denials. Better physician feedback shortens the correction cycle and improves coding consistency over time.
One trade-off deserves attention. Heavy pre-bill review can improve claim quality, but it can also slow final bill drop if every encounter goes through the same manual process. High-performing teams avoid that trap by routing only higher-risk accounts for deeper review, such as surgeries, infusion services, observation stays, and claims with frequent modifier use. Lower-risk professional claims can often move through automated edits with targeted exceptions.
For most organizations, the highest-yield fixes are not complicated. Standardized charge review queues, specialty-specific documentation templates, and a short weekly coder-clinician review session usually produce better results than broad annual retraining. Teams that want to reduce repeat corrections should also study medical coding errors that create avoidable rework so education stays tied to actual claim failure points.
Under-coding is another area leaders miss because it does not always trigger a denial. A claim may pass edits and still fail financially if the documentation supports a higher-acuity service, additional diagnosis specificity, or billable supply and procedure detail that never makes it onto the claim. That is why coding accuracy standards should measure both technical cleanliness and revenue integrity.
A useful operating model is simple. Set pre-bill edit rules. Audit a defined sample by specialty. Report error trends monthly. Require documented follow-up on repeat findings. Clean claim performance improves when standards are specific enough to manage and visible enough to enforce.
3. Proactive Claims Follow-Up and Management System
Most claim follow-up failures come from weak prioritization. Staff work the queue in the order claims appear, or they chase the loudest payer first. Neither method gives leadership control over cash.
A better system separates claims by financial risk, payer behavior, and filing deadlines. Clean electronic claims with normal adjudication patterns don't need the same attention as corrected claims, high-dollar procedures, or accounts sitting near timely filing limits. The goal isn't to touch every claim equally. It's to intervene where delay creates the biggest financial consequence.
Work the queue by risk, not by habit
The management system should be simple enough that staff can use it every day:
- Create aging buckets: Use standard buckets such as 0 to 30, 31 to 60, 61 to 90, and 90-plus days so leaders can see where delays accumulate.
- Set payer-specific follow-up rules: Some payers need an early status check. Others respond better after adjudication windows close.
- Document every touch: If a representative gave a reference number, promised reprocessing, or requested records, log it immediately.
- Escalate high-value claims faster: Large surgical, infusion, and facility claims shouldn't sit in the same workflow as low-balance routine encounters.
Claims follow-up works best when the team knows exactly which accounts deserve same-day action and which can wait.
A strong real-world pattern is using clearinghouse acknowledgments, electronic claim status responses, and work queues together. Teams that rely only on payer portals often lose time toggling between systems. Teams that combine status automation with a disciplined manual escalation path usually move faster because they aren't searching for the next action.
This is also where staffing design matters. High-performing groups don't assign the same person to every kind of follow-up. They split work by payer group, denial type, or balance threshold so experience compounds instead of scattering across a generalist queue.
4. Denial Management and Root Cause Analysis Program
Denials aren't just billing events. They're evidence that a process upstream failed. A missing authorization points back to scheduling or pre-cert. A registration mismatch points back to front-end intake. A medical necessity denial usually points to documentation, coding, or both. If your team only works denials after the payer rejects the claim, you're paying twice for the same mistake.
The strongest denial programs centralize every denial reason in one tracking system and classify them in a way operations leaders can act on. Broad categories help. Eligibility, authorization, coding, duplicate billing, noncovered services, documentation, and payer-specific edits are usually enough to identify where to intervene.
Treat denials as process failures, not billing noise
A denial program gets traction when it has structure:
- Log the full denial record: Patient, payer, claim, denial reason, filing deadline, and financial value should all be visible in one place.
- Split recoverable from nonrecoverable: Staff shouldn't spend the same energy on every denial.
- Review trends with operations leaders: Denial meetings need registration, coding, clinical, and finance representation.
- Write corrective actions by owner: “Improve authorization workflow” isn't a corrective action. “Pre-cert team verifies CPT list against scheduled procedure before date of service” is.
A common example is a surgery group with a steady stream of supply-related denials. Billing kept appealing them, but the root of the problem was payer contract interpretation and implant reimbursement rules. Once the team tied denial categories to contract terms and case costing, recovery improved and the same denials stopped recurring.
If you're trying to tighten this area, focused medical revenue recovery strategies usually outperform broad appeals campaigns because they direct effort toward denials with a clear contractual or documentation path to payment.
Field note: If the same denial reason appears month after month, stop asking the billing team to work harder. Ask which upstream process still hasn't changed.
5. Patient Financial Responsibility Management and Collections Strategy
Patient collections are easiest when the balance feels predictable and explainable. They become difficult when the first financial conversation happens after service, after adjudication, and after the patient has already received a confusing statement. Best practice revenue cycle management treats patient responsibility as a communication issue as much as a collections issue.
That starts with clear estimates, plain-language explanations, and a payment path that doesn't make patients call the office three times to resolve one bill. CFOs often focus on collection policy, but day-to-day execution usually matters more. Are estimates being delivered before service? Can staff explain deductible and coinsurance without jargon? Are payment plans easy to enroll in?

Make the patient balance understandable and collectible
Operationally, a strong patient collections model usually includes:
- Pre-service estimates when possible: Especially for elective and scheduled services.
- Multiple payment channels: Portal, phone, mailed payment, card on file where appropriate, and structured payment plans.
- Statement timing that matches reality: Don't let balances sit without communication while patients forget the encounter.
- Financial assistance routing: Staff should know when to collect, when to counsel, and when to redirect to assistance screening.
One scenario plays out constantly in practices with growing deductible exposure. The payer eventually processes the claim correctly, but the patient rejects the balance because no one prepared them for it. The bill may be valid, yet the account still ages because the communication failed. That isn't a collections failure. It's a front-end failure showing up late.
Plain language matters here more than many executives expect. Replace insurer terminology with short explanations. Tell the patient what was billed, what the payer processed, what remains, and what options exist. Collections usually improve when the statement reads like a conversation instead of a remittance advice.
6. Payer Contract Management and Fee Schedule Optimization
Many organizations negotiate payer contracts and then barely operationalize them. The agreement gets stored, fee schedules get loaded, and everyone assumes reimbursement will take care of itself. It doesn't. Contract performance has to be monitored the same way claim edits and denials are monitored.
This is especially important in procedural and surgical settings where supplies and implants materially affect reimbursement. A frequently missed issue is whether contracted insurance agreements reimburse implants at cost or at a percentage. The Revenue Cycle Management Best Practices Guide for Rural Centers specifically notes that practices must verify whether supplies are reimbursed at cost or only a percentage to determine proper bill markup. Many mainstream optimization discussions barely address this, even though supplemental supply and implant cost verification can represent 15 to 25 percent of total surgical revenue.
Read the contract language that affects real reimbursement
What strong contract management looks like in practice:
- Maintain a contract calendar: Know renewal dates, amendment windows, and notice periods.
- Audit fee schedules after every change: Loaded rates often drift from signed terms.
- Review underpayments systematically: Compare expected reimbursement to actual payment at the CPT and payer level.
- Check supply and implant language before billing: Especially in orthopedics, ASC cases, pain, and device-heavy specialties.
One practical example is the surgery center that billed implants using a default markup because no one had verified whether the payer reimbursed at cost or by percentage. Claims weren't necessarily denied outright, but net revenue was wrong. Once contract terms were reviewed alongside case costing, the team could bill consistently and appeal from a stronger position when payment didn't match the agreement.
This area rewards detail-oriented finance and RCM collaboration. Contract terms live on paper, but reimbursement accuracy lives in operations. If those teams don't meet, fee schedule optimization stays theoretical.
7. Revenue Cycle Technology Integration and Data Analytics
A significant share of revenue cycle loss starts with fragmented workflows, not payer behavior. Registration data sits in one system, claim edits in another, denials in a third, and reporting arrives too late to prevent the next error.
RCM technology should reduce handoffs and give operators one dependable view of performance across eligibility, coding, claim submission, denial management, payment posting, and reporting. When those functions sit in disconnected tools, staff spend hours reconciling files, correcting mismatched statuses, and debating whose numbers are right. That work adds cost without improving collections.
As noted earlier, investment in AI and automation is rising across RCM. The practical takeaway is not that every organization needs a new platform. It is that practices need a stack that supports faster decisions, cleaner data flow, and earlier intervention on accounts likely to go off track.
A quick visual overview helps frame what integrated reporting should support:
Use integrated systems to reduce handoffs and blind spots
Strong integration changes management behavior. Leaders can review the same numbers every week, trace a denial trend back to registration or coding, and assign ownership before a problem spreads across another month of claims.
In practice, a workable setup usually includes an EHR or practice management system, clearinghouse connectivity, rules-based claim edits, denial categorization, payment posting controls, and reporting that drills from high-level KPIs down to account detail. The trade-off is real. More tools can add useful features, but each additional handoff increases the risk of delayed data, duplicate work, and conflicting reports.
Use this playbook to judge whether technology is helping operations or just adding complexity:
- Start with interoperability. Data from registration, billing, and payments must sync reliably before new features matter.
- Define the metric owner. Every dashboard KPI needs a person responsible for review, action, and follow-up.
- Reconcile source data routinely. Compare dashboard totals against posted charges, remittances, and bank activity so reporting errors do not drive bad decisions.
- Use analytics for prevention. Flag authorization gaps, demographic errors, coding mismatches, and high-risk claims before submission.
- Set drill-down expectations. Executives need trend views. Managers need work queues. Staff need account-level detail they can act on the same day.
One common example is a multispecialty group that tracks denials by payer but cannot tie those denials back to location, registrar, or rendering provider. The report looks useful, but it does not support correction. Once the denial data is mapped to front-end and coding inputs, the team can identify whether the problem is eligibility, authorization, documentation, or edit logic and fix the right workflow.
Organizations that want more visibility often start with healthcare revenue cycle analytics that connect operational data to financial action. At that point, best practice revenue cycle management stops being a checklist and becomes a control system.
8. Compliance and Risk Management in Revenue Cycle Operations
Compliance can't sit in a separate silo from revenue cycle operations. Billing rules, documentation standards, payer requirements, privacy obligations, refund handling, and segregation of duties all affect whether revenue is sustainable. A claim that gets paid today can still create risk later if the documentation doesn't support it or the billing workflow isn't controlled.
The strongest programs build compliance into daily operations. They don't wait for an annual review to discover recurring issues. They define who can enter charges, who can post payments, who can approve adjustments, and how decisions are documented. That's basic control design, but many practices still operate informally until an audit exposes the gaps.
Audit more often if you want better financial control
New evidence makes the case for more frequent review. A Journal of Healthcare Financial Management finding summarized in Inovalon's discussion of revenue cycle best practices reported that practices conducting quarterly RCM self-assessments improved net revenue by 7.3% over 12 months, while annual-only auditors improved by 2.1%. The same evidence also indicates quarterly reviews reduce Days in A/R by 12 to 18% and increase clean claim rates by 9% compared with annual-only audits.
That matters because compliance reviews aren't just about avoiding penalties. They improve financial control when they catch documentation gaps, adjustment patterns, posting inconsistencies, and billing rule drift before those issues spread.
Review a small, representative sample every quarter and act on the findings immediately. Annual audits are too slow for a fast-changing payer environment.
A practical compliance structure usually includes:
- A cross-functional committee: Billing, operations, clinical leadership, and compliance should all be represented.
- Written billing policies: Staff need one current source of truth.
- Segregation of duties: Approval, posting, and follow-up shouldn't sit with one person when avoidable.
- Quarterly audit cadence: Frequent review creates faster correction loops than annual-only oversight.
8-Point Revenue Cycle Management Comparison
| Solution | Implementation Complexity 🔄 | Resource Requirements 💡 | Expected Outcomes ⭐📊 | Ideal Use Cases | Key Advantages ⚡ |
|---|---|---|---|---|---|
| Front-End Revenue Cycle Optimization (Registration & Eligibility Verification) | Medium–High: real-time integrations and workflow redesign | EHR integration, eligibility vendors, trained registration staff | Reduces denials 25–40%; higher first-pass acceptance; lower A/R days | High-volume ambulatory clinics; organizations with frequent coverage gaps | Prevents avoidable denials; improves upfront collections; better cash flow |
| Clean Claim Submission & Coding Accuracy Standards | Medium: process controls, audits, ongoing training | Coding software, certified coders, audit tools | Clean claim rate 95%+; fewer rejections; improved compliance | Practices with complex coding or high claim volumes | High first-pass accuracy; lower rework costs; stronger compliance |
| Proactive Claims Follow-Up & Management System | Medium: automation plus payer-specific workflows | Claims tracking platform, dedicated follow-up staff | Reduces DSO ~20–30%; faster claim resolution; fewer aged claims | Organizations with aging AR or slow payer responses | Faster recoveries; targeted escalation for high-dollar claims |
| Denial Management & Root Cause Analysis Program | High: analytics, cross-department process changes | Centralized denial system, analysts, appeals team | Reduces denial rates 30–50%; recovers preventable revenue via appeals | Systems with recurring denials or high denial costs | Identifies root causes; prevents recurrence; improves operations |
| Patient Financial Responsibility Management & Collections Strategy | Medium: policy design and patient-facing workflows | Estimation tools, payment portals, trained financial counselors | Improves patient collections 15–25%; reduces bad debt | Practices with significant patient OOP responsibility | Increases upfront collections; enhances patient transparency and satisfaction |
| Payer Contract Management & Fee Schedule Optimization | High: detailed contract analysis and negotiation | Contract analysts, benchmarking tools, ERA analysis | Recovers 2–5%+ revenue from underpayments; improves rates | Multi-payer environments and larger practices | Recovers underpayments; strengthens negotiation leverage |
| Revenue Cycle Technology Integration & Data Analytics | High: complex integrations, data governance | Integrated platforms, BI tools, IT/analytics staff | Real-time KPI visibility; predictive denial detection; higher productivity | Organizations scaling operations or needing data-driven decisions | Automation of workflows; actionable dashboards; predictive insights |
| Compliance & Risk Management in Revenue Cycle Operations | Medium–High: continual monitoring and controls | Compliance officers, audit programs, training resources | Reduces regulatory risk and penalties; improves billing accuracy | Any organization subject to HIPAA/CMS audits and fraud risk | Protects against fines; prevents fraud; ensures proper documentation |
From Best Practices to Better Performance
Mastering the revenue cycle doesn't come from optimizing one isolated function. It comes from building a system where each part reinforces the next. Registration accuracy makes coding easier. Better coding produces cleaner claims. Cleaner claims reduce denials. Strong denial analysis improves the front end and mid-cycle. Contract oversight protects the reimbursement you expected to receive. Analytics show where the process is slipping, and compliance audits make sure short-term fixes don't create long-term risk.
That's why best practice revenue cycle management is less about individual tactics and more about operating discipline. Most organizations already know the broad categories they should improve. What they often lack is a practical playbook, clear ownership, and the consistency to review performance often enough to change outcomes. The difference between an average revenue cycle and a strong one usually isn't awareness. It's execution.
The organizations that improve fastest tend to do a few things well. They simplify workflows instead of layering on workarounds. They standardize how staff handle exceptions. They give leaders visibility into payer-specific and workflow-specific problems. And they don't let denials, underpayments, or patient balances drift until month-end reporting exposes the damage.
They also understand the trade-off between patching problems internally and getting outside help. Some practices have the staff and systems to tighten one weak area on their own. Others need a partner because the problems are spread across benefit verification, payment posting, follow-up, coding coordination, and reporting. In both cases, the right next step is an honest assessment of where the leakage starts and who owns the fix.
At Clarity Health RCM, we help providers turn these revenue cycle best practices into working processes. That may mean supporting your full operation end to end, or strengthening a specific gap such as insurance benefit verification, claims follow-up, payment posting, or fee schedule setup. The right model depends on your staffing, specialty mix, payer complexity, and growth goals.
If your leadership team wants stronger financial performance without pulling physicians and administrators deeper into billing complexity, start with a practical review of the current state. The quickest gains usually come from a few targeted operational changes, not a wholesale overhaul. Once those are in place, the revenue cycle becomes easier to manage, easier to measure, and far more supportive of patient care.
If you're ready to strengthen collections, reduce avoidable rework, and build a more reliable financial operation, Clarity can help. We provide full-service and a la carte healthcare revenue cycle support, including fee schedule and practice management setup, billing operations support, insurance benefit verification, and claim status and payment posting. It starts with a complimentary consultation of your current revenue cycle so we can recommend a customized plan that fits your practice.
No responses yet