If you're leading a practice right now, you've probably felt this disconnect. Visit volume looks stable. Providers are busy. Claims are going out. Yet Medicare Advantage revenue still shifts in ways that don't line up neatly with your scheduling, charge capture, or denial reports.
That usually means you're looking at the wrong dashboard.
In fee-for-service, leaders could often explain performance with familiar metrics: charges, collections, lag days, denials, and payer mix. In value-based reimbursement, those indicators still matter, but they don't tell the full story. A patient panel's documented complexity now carries financial weight, and when that complexity isn't captured correctly, revenue drifts away unnoticed. The loss rarely shows up as a dramatic rejected claim. It shows up as underpaid future reimbursement, weak benchmarking, and audit exposure you only discover later.
That's where the answer to what is RAF score becomes operational, not academic. RAF is one of the hidden metrics behind Medicare Advantage payment accuracy. If your team treats it as a coding side topic, you'll miss two of the biggest leak points in modern revenue cycle performance: documentation that doesn't support the diagnosis with MEAT evidence, and outdated assumptions about the new CMS-HCC model changes.
Table of Contents
- The Hidden Metric Driving Your Practice Revenue
- Decoding the RAF Score Components
- How CMS Calculates and Adjusts RAF Scores
- The Financial Impact of Accurate RAF Scores
- Navigating Compliance Risks and Audit Triggers
- Actionable Strategies to Improve RAF Score Accuracy
The Hidden Metric Driving Your Practice Revenue
A common scenario looks like this. A medical group reviews month-end performance and sees that Medicare Advantage payments don't match the apparent workload of the panel. One physician feels like she manages a very sick population, but payer reimbursement doesn't seem to reflect it. Another provider's panel appears financially stronger, even though the clinical burden doesn't look dramatically different on the surface.
The gap often comes down to how well the chart tells the patient's story.
RAF score stands for risk adjustment factor, and CMS uses risk adjustment to estimate the expected cost of caring for a beneficiary relative to the average Medicare patient. In plain terms, the score is a pricing signal attached to documented clinical complexity. It helps determine how Medicare Advantage plans are paid, which is why it has such a direct downstream effect on provider economics in risk-based arrangements and value-oriented contracts.
If you want a simple analogy, think of RAF as the practice's translation layer between clinical reality and financial recognition. If that translation is incomplete, your patient population can be more complex than your reimbursement suggests. If that translation is overstated or unsupported, you'll invite compliance trouble.
That is why old-school RCM visibility isn't enough anymore. Clean claims and low A/R don't protect revenue when the underlying illness burden is undercaptured. Strong front-end and back-end operations still matter, but leadership also needs a risk-adjustment lens alongside healthcare revenue cycle analytics.
Payments can look inconsistent when the real issue isn't claim execution. It's documentation fidelity across the patient panel.
For busy practice leaders, the practical question isn't just "what is RAF score." It's this: does your documentation and coding process produce a score that is both complete and defensible?
Those two words matter. Complete protects revenue. Defensible protects compliance.
Decoding the RAF Score Components
The clearest way to answer what is RAF score at the component level is to look at what CMS rewards, what it ignores, and where practices lose money. RAF is built from demographic data plus documented conditions that map to HCCs. Revenue leakage usually starts in two places. A condition is present but not supported with MEAT, or the diagnosis was captured under an older documentation habit that does not hold up well under CMS-HCC V28.
CMS defines a risk score as a number representing the predicted cost of treating a specific patient or group compared with the average Medicare patient. In day-to-day operations, 1.0 is commonly used as the baseline for the average Medicare beneficiary. Scores above that suggest higher expected cost, and scores below it suggest lower expected cost, as described by CMS risk adjustment guidance.
For leadership, the practical issue is simple. RAF is the payment model's summary of patient complexity, but only the complexity that is documented, coded, and accepted by the CMS model counts.
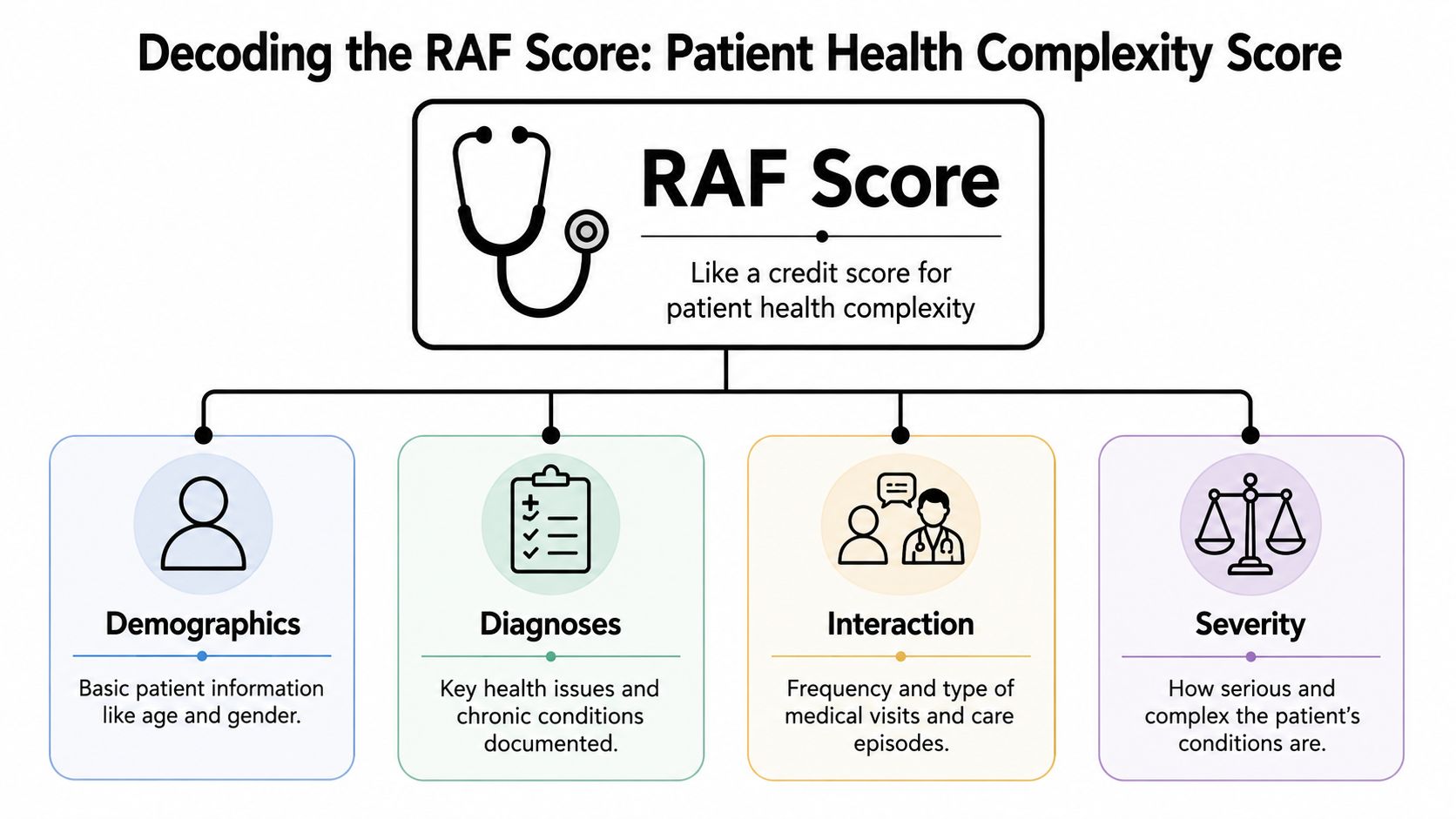
What goes into the score
RAF is built from a few core inputs, but their weight is not equal.
- Demographic factors. CMS uses age, sex, Medicaid status, disability status, and residence setting to set part of the expected cost baseline.
- Diagnosis data tied to HCCs. ICD-10 diagnoses map to Hierarchical Condition Categories, which group related conditions by expected clinical and financial burden.
- Disease interactions and severity logic. Some conditions carry more weight because of severity, and some combinations change the risk picture when they occur together.
- Model-year rules. The same charting habits do not always produce the same result from one CMS-HCC version to the next, which is why V28 deserves attention from both coding and compliance teams.
A longer problem list does not guarantee a stronger RAF score. CMS pays for supported burden, not diagnosis volume. If diabetes is documented without status, complications, or active management, the note may reflect clinical reality poorly and the code may carry less risk value than the patient warrants. If chronic conditions are listed with no clear MEAT support, the risk goes beyond missed revenue. It creates audit exposure because the diagnosis lacks a defensible treatment story.
That is why MEAT matters so much. Monitoring, evaluating, assessing or addressing, and treating are not documentation formalities. They are the evidence that a condition affected care during the encounter year. In practice, many undercoded charts have the condition name but not the management detail. Many overexposed charts have the opposite problem. A diagnosis is carried forward with weak support.
This table gives leaders the shortest useful view:
| Component | What it captures | Why leaders should care |
|---|---|---|
| Demographics | Patient attributes recognized by the model | These set part of the baseline expected cost |
| HCC-mapped diagnoses | Active, documented conditions translated from ICD-10 into HCC categories | Specificity, annual recapture, and coding accuracy affect payment |
| Interaction and severity logic | Higher-burden presentations and certain condition combinations | These can materially change the score beyond a simple condition count |
| Documentation support | MEAT tied to each reported condition | This protects both revenue integrity and audit defensibility |
HCCs work like disease families with ranking rules. Related diagnoses do not always stack. In many cases, the more severe manifestation overrides the less severe one within the same hierarchy. That is a common source of confusion for operators who expect every diagnosis to add value independently.
Practical rule: If the note does not show how the condition was monitored, evaluated, assessed, addressed, or treated, the RAF score may not reflect the cost of caring for that patient, and the code may not survive review.
Routine medical coding errors that distort risk adjustment and future payment accuracy cost more than a single claim rework. They can suppress the documented illness burden across the panel, especially when teams fail to refresh coding and documentation habits for CMS-HCC V28.
How CMS Calculates and Adjusts RAF Scores
From encounter to risk score
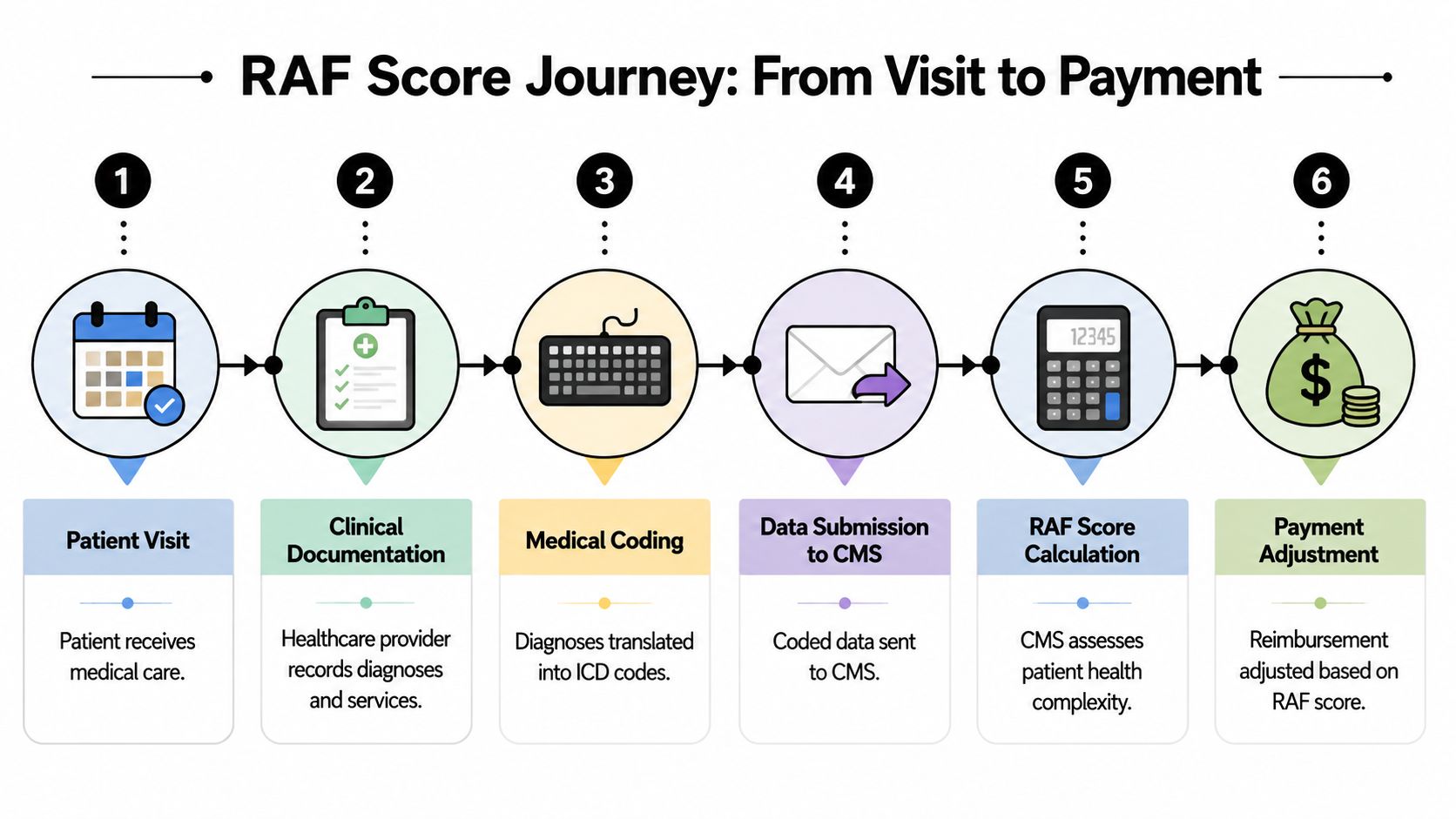
The path from office visit to reimbursement isn't mysterious, but a lot of teams treat it like a black box. In practice, the sequence is straightforward.
- The patient is seen. A face-to-face encounter occurs.
- The provider documents active conditions. The note needs to reflect what was addressed and how it was managed.
- The diagnoses are coded. ICD-10 codes are assigned based on the documentation.
- The codes map to HCCs. CMS uses these mapped categories, along with demographic inputs, to calculate risk.
- The payment effect happens later. CMS uses claims and encounter data retrospectively to determine the risk score for future payment periods.
That retrospective feature is one of the most misunderstood parts of RAF. Teams often expect immediate visit-level financial impact. Risk adjustment doesn't work that way. Documentation captured during care contributes to a score used for later payment calculation, which is why annual recapture discipline matters so much.
A strong grasp of this workflow also helps leaders understand where a breakdown occurs. Sometimes the note is vague. Sometimes the code doesn't reflect the specificity in the note. Sometimes the claim process is fine, but the risk signal was weak from the moment the provider closed the encounter. That's why concepts like claim adjudication matter operationally, even though RAF itself isn't just a front-end claims issue.
Later in the workflow, this overview can help orient clinical and finance teams:
Why more codes do not always mean more value
RAF isn't a stacking game. The model applies hierarchy rules, meaning when multiple related conditions fall within the same disease hierarchy, only the most severe HCC contributes. That prevents double counting of related burden, as explained in IMO Health's RAF overview.
Some documentation improvement efforts go off track. Leaders push for "capturing more," and the organization responds by adding more diagnoses without improving specificity. That rarely creates the result they expect.
A short comparison makes the point clear:
| Documentation behavior | What happens |
|---|---|
| Lists broad, less specific related conditions | May fail to reflect the highest supported severity |
| Documents the clinically supported, most specific condition | Better aligns with hierarchy logic |
| Adds redundant related diagnoses in the same family | Doesn't necessarily increase RAF value |
Why timing matters more than most teams expect
Retrospective scoring changes management priorities. The visit you're documenting today may influence how the population is valued in the next payment cycle. That creates a very different operating cadence from fee-for-service billing.
It also explains why missed chronic condition recapture can be so costly without creating obvious noise in daily operations. There may be no immediate denial. No conspicuous hard stop. Just a weaker risk profile later.
Accurate RAF work is less like chasing one claim and more like maintaining an annual inventory of clinically managed disease burden.
The Financial Impact of Accurate RAF Scores
Where the money is actually won or lost
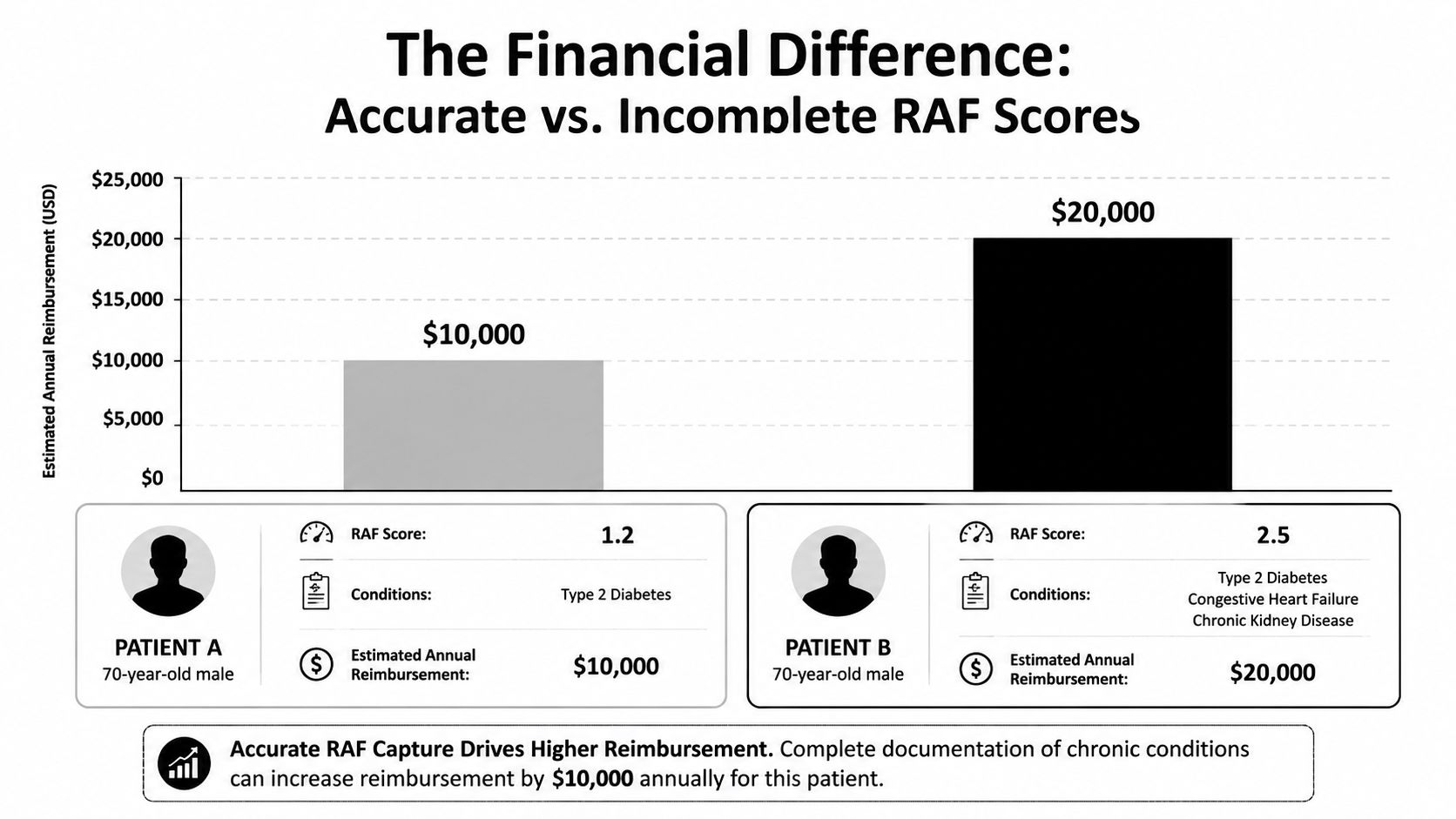
The biggest misunderstanding in leadership meetings is that RAF is a coding department issue. It isn't. It's a revenue recognition issue tied to how thoroughly the organization converts clinical complexity into supportable documentation.
You don't need invented case-study math to see the pattern. Consider two patients who look similar at a glance because both have diabetes. If one chart documents only a generic diabetic diagnosis and the other clearly supports diabetes plus additional active chronic conditions that are being managed, those records won't tell the same financial story. One chart reflects a simpler patient than the provider may be managing.
That difference affects more than reimbursement optics. It changes forecasting, payer performance comparisons, provider panel analysis, and confidence in contract economics.
A practical comparison without fantasy math
Here's the practical way I advise leaders to frame it.
| Patient profile | Documentation quality | Likely RAF effect |
|---|---|---|
| Diabetes noted in a general way | Broad and incomplete | Lower representation of expected cost burden |
| Diabetes documented with supported related chronic complexity | Specific and clinically traceable | More accurate representation of expected cost burden |
The problem is rarely that clinicians fail to treat complexity. The problem is that complexity often appears in fragmented language across the chart. The nephrology issue sits in one note, the heart failure status in another, and the primary care encounter doesn't clearly show active management. Financially, fragmented truth behaves a lot like missing truth.
For finance leaders, the trade-off is straightforward:
- Under-document supported complexity and you risk underpayment.
- Overstate unsupported complexity and you risk recoupment.
- Document precisely with clinical traceability and you give the organization a better shot at revenue integrity.
A complete RAF picture doesn't inflate payment. It aligns payment with the burden your clinicians are already carrying.
Practices that improve RAF accuracy usually don't start by asking coders to work faster. They start by tightening the handoff between clinician thought process, note construction, diagnosis specificity, and coder validation. That's where financial performance changes in a durable way.
Navigating Compliance Risks and Audit Triggers

The fastest way to create compliance risk is to treat RAF as a score-maximization exercise. CMS doesn't pay for a diagnosis because it appears on a problem list. The condition has to be supported in the patient encounter, and the note has to show that the condition was actively managed.
That is where many organizations are exposed. A 2024 CMS audit report found that nearly 18% of denied RAF adjustments were tied to insufficient documentation linking diagnoses to patient encounters, and CMS requires evidence that the diagnosis was actively managed through MEAT: Monitoring, Evaluation, Assessment, and Treatment.
MEAT is the difference between supportable and exposed
MEAT is the operational filter that turns a diagnosis from a mention into a defensible condition.
- Monitoring means the clinician is tracking the condition, symptoms, progression, labs, or status.
- Evaluation means reviewing data, testing, response, or relevant findings.
- Assessment means the provider makes a judgment about current status, stability, progression, or significance.
- Treatment means there is an active plan, medication management, referral, follow-up, or other intervention.
A useful analogy is that HCC coding tells you the label on the file, but MEAT tells you whether anyone opened the file and did the work.
Weak note versus defensible note
A weak note for a chronic condition might read like this:
CHF. Diabetes. Continue meds.
That may reflect real illness, but it doesn't show enough management activity to support the diagnosis well in an audit context.
A stronger note sounds different:
Assessment: Chronic systolic heart failure, symptomatic with ongoing medication management. Monitoring/Evaluation: Reviewed symptoms and current medication tolerance. Treatment: Continue current regimen and follow up on response.
Assessment: Type 2 diabetes with ongoing management. Monitoring/Evaluation: Reviewed current control and related clinical status. Treatment: Continue treatment plan and reinforce follow-up.
The point isn't to turn every note into a legal brief. The point is to make the evidence chain visible.
Here are the common audit-trigger behaviors I see most often:
- Problem-list carryforward. The diagnosis stays in the chart, but the encounter doesn't show active management.
- Generic language. Terms are too vague for a coder or auditor to connect clearly to supported severity.
- Disconnected records. The condition is clinically real, but the support sits in scattered places and doesn't tie back to the encounter.
- Template overuse. Notes repeat stock phrases without showing patient-specific management.
Leaders should treat unsupported RAF capture the same way they treat unsupported charges. If you can't defend it from the record, it isn't stable revenue.
Actionable Strategies to Improve RAF Score Accuracy
Build a workflow clinicians will actually use
Most RAF improvement plans fail because they add theory instead of changing workflow. Busy physicians won't adopt a process that feels like a second job, and coders can't fix what never made it into the note.
The strongest approach is operationally simple.
- Run pre-visit chart review for chronic conditions. Give clinicians a focused view of likely recapture opportunities before the patient arrives.
- Use EHR templates carefully. Prompts should support specificity and active management, not encourage copied language.
- Create coder-to-provider feedback loops. When coders see unsupported or vague diagnoses, they need a clean query path back to the clinician.
- Train around note quality, not just code lists. Providers usually don't need a lecture on HCC theory. They need examples of how to document active disease management clearly.
- Review high-complexity encounters first. Not every chart carries the same RAF impact, so prioritize the records where chronic burden and specificity matter most.
This is also where leadership alignment matters. The CMO, CFO, compliance lead, and coding manager shouldn't be working from separate definitions of success. Revenue wants completeness. Compliance wants support. Clinical operations want speed. A workable RAF process respects all three.
The best RAF workflow doesn't ask clinicians to become coders. It helps clinicians document care in a way coders can defend.
Prepare your finance team for V28 reality
The second major blind spot is model change.
CMS-HCC Version 28, effective October 2024, is expected to alter RAF score predictability. An independent analysis projects that 12 to 15% of Medicare Advantage RAF scores may shift because of new HCC additions and coefficient changes, making older benchmarks less reliable and requiring recalibration of risk models.
That matters for more than coding education. It affects finance.
A practical V28 response includes:
- Revisit benchmarking assumptions. Historical trends may no longer compare cleanly across periods.
- Reassess contract modeling. If your team still uses pre-V28 expectations as if nothing changed, forecasts can drift.
- Update provider education. Old documentation habits may no longer align cleanly with the revised model.
- Separate operational misses from model-driven movement. Not every score change reflects poor performance. Some reflect structural change in the model itself.
When leaders ask what is RAF score, the strategic answer is: it's a reimbursement signal that only works when documentation, coding, compliance, and financial planning are all synchronized. Miss the MEAT standard and you risk denials or recoupment. Ignore V28 and you risk making decisions from stale assumptions.
If your organization needs help tightening documentation, coding workflows, and revenue visibility around RAF performance, Clarity can help evaluate the gaps in your current revenue cycle and build a practical plan that supports both reimbursement accuracy and compliance.
No responses yet