Your appointment slot says 60 minutes. But under CMS billing rules, the actual time threshold for CPT 90837, individual psychotherapy at the "60-minute" level, starts at 53 minutes, not 60. A session where you provided 54 minutes of psychotherapy and a session where you provided 58 minutes both map to the same code. What changes which code you bill is whether the documented psychotherapy time crossed that 53-minute line.
At Clarity Health RCM, we support mental and behavioral health billing among the specialties we serve. CPT 90837 is one of the codes we see most frequently misunderstood, not because providers are billing fraudulently, but because the gap between what the code is called and what the billing rules actually require creates real exposure for practices that don't know where the line is.
This guide covers exactly where that line is, what your documentation needs to contain, why payers scrutinize 90837 more than most psychotherapy codes, and how to handle the edge cases – add-on codes, telehealth modifiers, prior authorization, and the scenarios where 90837 is the wrong code entirely. By the end, you'll have a clear picture of what makes a 90837 claim defensible and what makes one a target.
What CPT 90837 covers, and when to use a different code
CPT 90837 is the American Medical Association's code for individual psychotherapy at the 60-minute level. The AMA describes it as a face-to-face therapeutic service involving assessment of mental status and symptom complexity, and therapeutic communication and methods intended to reduce emotional distress and morbidity. (American Medical Association)
It is a standalone psychotherapy code – meaning it is billed by itself, for a psychotherapy-only encounter, when there is no separate evaluation and management service on the same date.
Three related distinctions matter immediately:
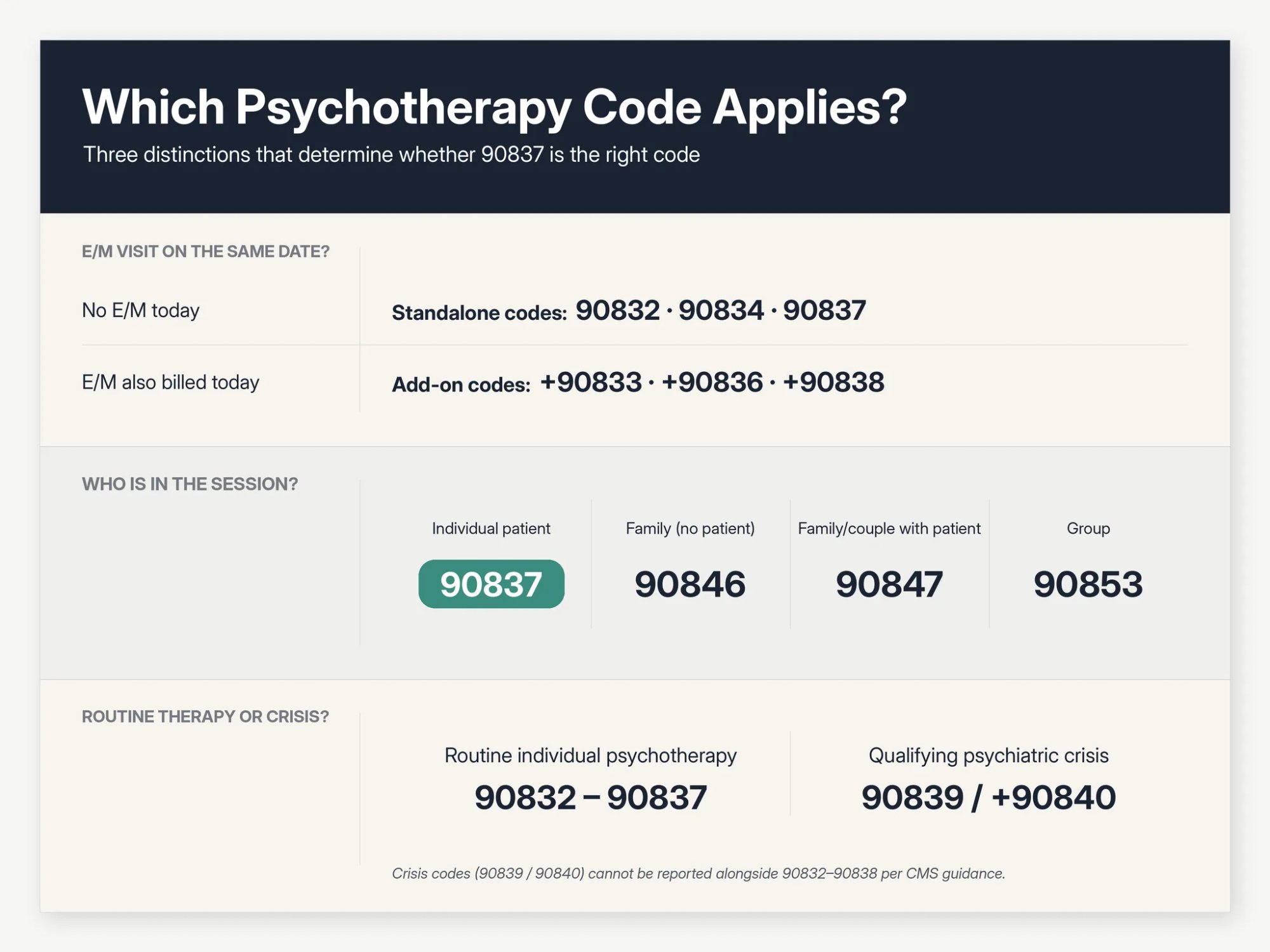
Standalone vs. add-on. When psychotherapy occurs without any E/M service, you use the standalone codes: 90832, 90834, or 90837. When psychotherapy occurs with a separately identifiable E/M service on the same date, as happens in psychiatry or with prescribers who both manage medications and provide therapy. You use the E/M code plus a psychotherapy add-on code. The standalone 90837 and the E/M-paired psychotherapy codes are different and not interchangeable.
Individual vs. family vs. group. CPT 90837 is for individual psychotherapy. Family psychotherapy without the patient present is 90846. Family psychotherapy with the patient present (when the family or couple system is the treatment focus) is 90847. Group psychotherapy is 90853. If you are billing for a family or group session and reaching for 90837, stop: the service you provided likely has its own code.
Psychotherapy vs. crisis. CPT 90837 is for routine individual psychotherapy, including intensive or complex psychotherapy for severe clinical presentations. It is not interchangeable with the crisis psychotherapy codes 90839 and +90840. CMS guidance is explicit that crisis codes should not be reported with 90832 through 90838. (CMS) If a patient's session escalates to a qualifying psychiatric crisis requiring urgent stabilization and disposition, a different code family applies.
Most therapists billing outpatient individual psychotherapy are billing the right type of service for 90837, the question is usually whether the time and documentation are sufficient.
CPT 90837 time requirement: 53 minutes, not 60
This is the single most important technical fact about 90837, and the one most providers don't have exactly right.
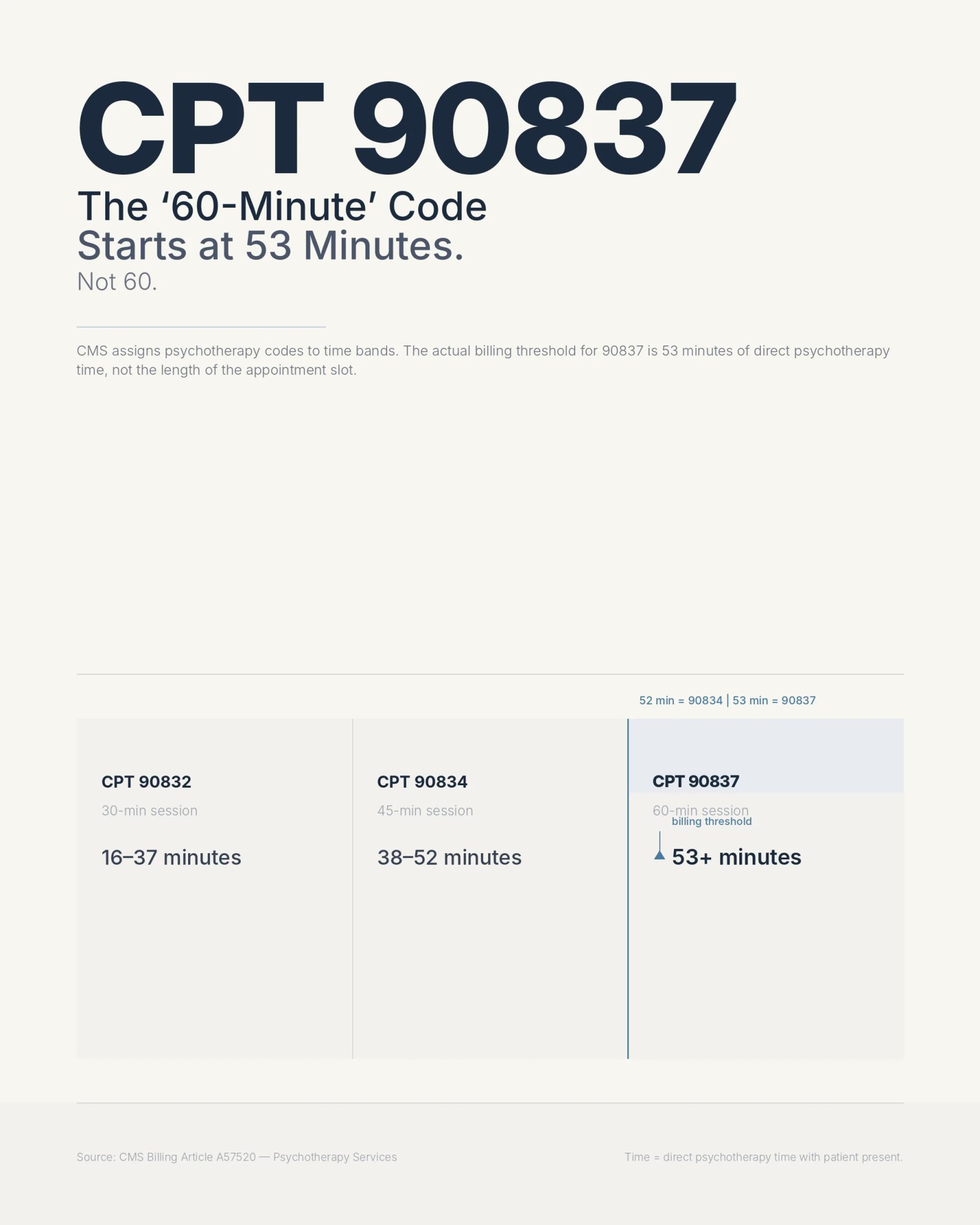
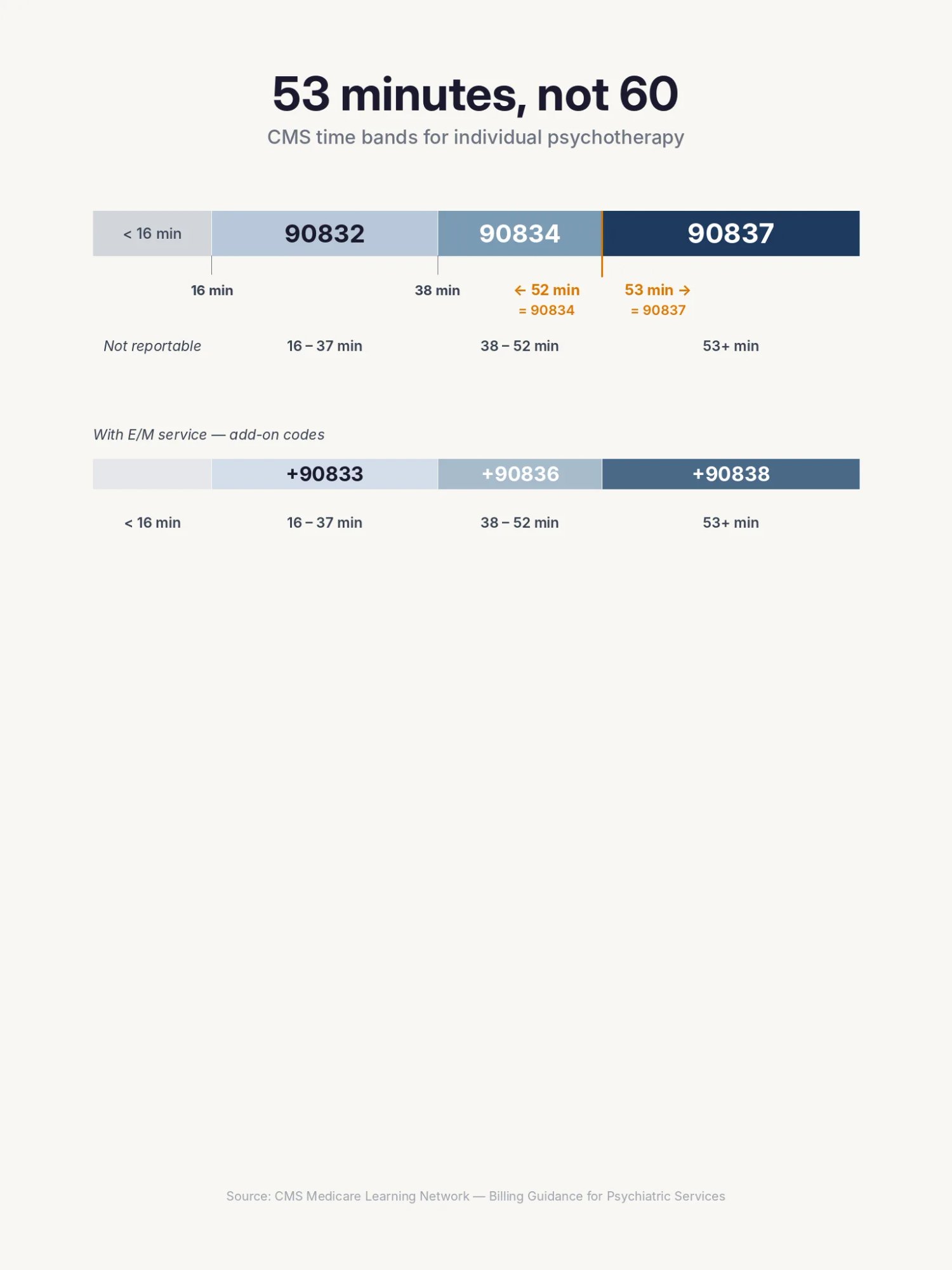
CMS assigns individual psychotherapy codes to time bands, and the bands for the standalone codes are: (CMS)
| Code | Common label | Actual psychotherapy time |
|---|---|---|
| 90832 | 30-minute psychotherapy | 16-37 minutes |
| 90834 | 45-minute psychotherapy | 38-52 minutes |
| 90837 | 60-minute psychotherapy | 53+ minutes |
And for psychotherapy provided with an E/M service, the add-on codes:
| Add-on code | Common label | Actual psychotherapy time |
|---|---|---|
| +90833 | 30-minute add-on | 16-37 minutes |
| +90836 | 45-minute add-on | 38-52 minutes |
| +90838 | 60-minute add-on | 53+ minutes |
Two boundaries to know cold:
52 minutes is 90834, not 90837. Even if the session was one minute short of the 90837 threshold, even if the patient's presentation was complex and the work was clinically intensive, 52 minutes maps to 90834. There is no rounding up.
53 minutes is 90837, provided medical necessity supports the extended session. You don't need 60 minutes on the clock. A 53-minute session with documented time and clinical justification is a legitimate 90837.
Does the 8-minute rule apply to 90837?
Physical therapy and occupational therapy use a unit-based "8-minute rule" to calculate timed units. Psychotherapy does not work this way. CPT 90837 and its siblings use the time-band structure above: you pick the code closest to the actual psychotherapy time, and the time must be documented. There is no mechanism in psychotherapy coding to accumulate partial units or round up to the next band. CMS states plainly that providers should select the code closest to the actual psychotherapy time. (CMS)
One more hard rule: if the psychotherapy time is less than 16 minutes, do not bill 90832, 90834, or 90837. There is no reportable standalone psychotherapy code below the 16-minute floor.
The time bands tell you which code to use. What they don't tell you is exactly what counts toward that time, and that is where most billing errors actually happen.
What counts as psychotherapy time for 90837?
The time you document for 90837 is direct psychotherapy time with the patient. That sounds simple, but a significant number of audited claims fail because the documented time included activities that don't count.
Activities that count toward psychotherapy time
Direct psychotherapy time includes time during which you are actively providing psychotherapy to the patient, with or without clinically appropriate participation by a family member or caregiver. Examples include:
- Individual CBT, DBT, psychodynamic therapy, trauma-focused therapy, motivational interviewing, exposure and response prevention, relapse-prevention therapy, or supportive psychotherapy
- Synchronous telehealth psychotherapy when payer requirements are met
- Time with a parent, spouse, guardian, or caregiver when it is part of the individual session and the patient is present for all or some of that time
- Clinically necessary safety planning, grounding, trauma processing, exposure work, coping-skills practice, and symptom stabilization performed as psychotherapy
CMS guidance establishes that psychotherapy times are face-to-face with the patient, and the patient must be present for all or some of the service. (CMS)
Activities that do not count toward psychotherapy time
Do not count:
- Time spent waiting for the patient
- Front-desk check-in
- Scheduling conversations
- Billing discussions
- Documentation you write after the patient leaves
- Chart review outside the direct psychotherapy service
- Prior authorization phone calls
- Time spent on E/M medication management when psychotherapy is provided alongside an E/M visit
- Missed-session time
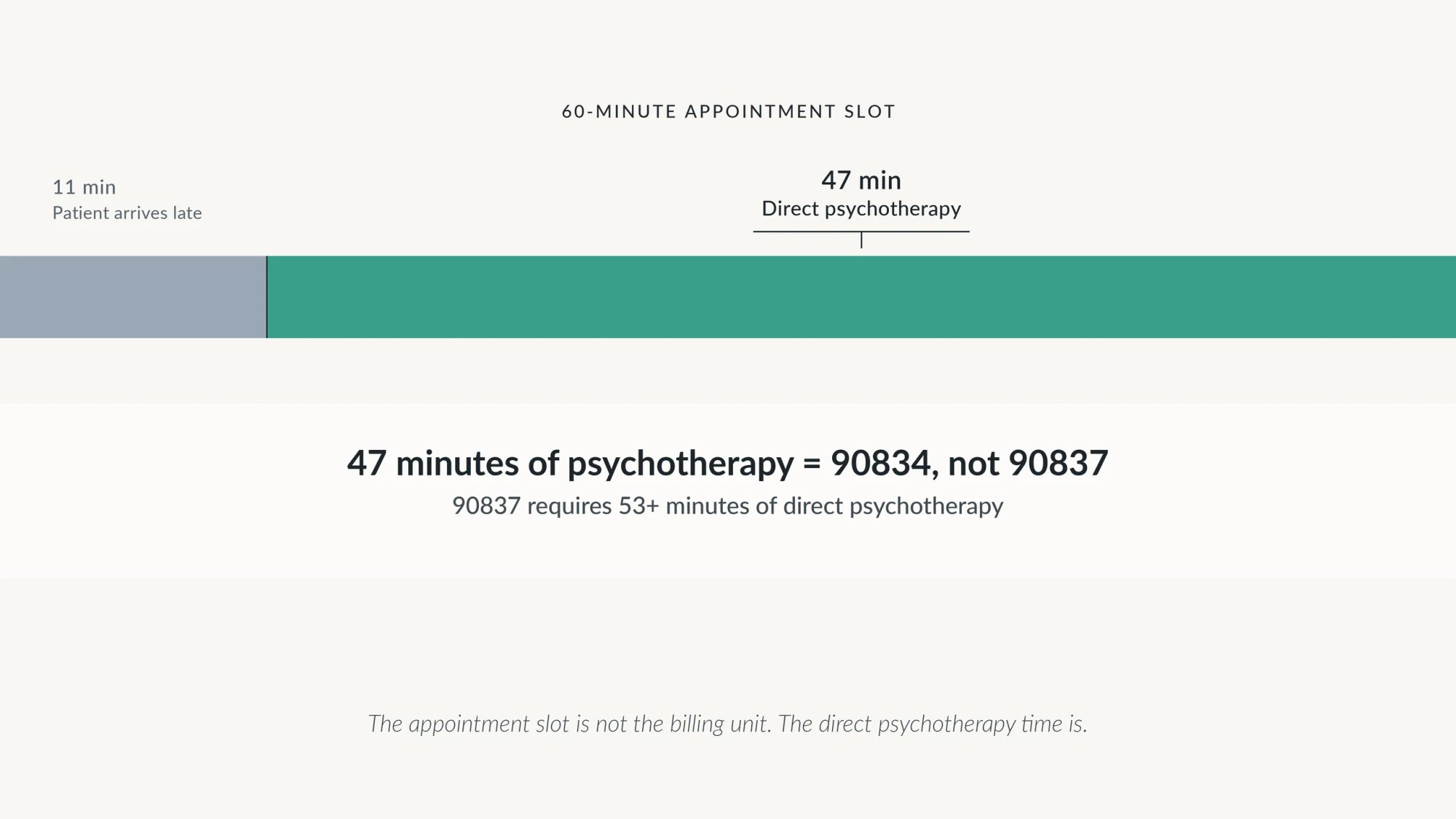
A concrete example illustrates why this matters: A patient has a 60-minute appointment slot. They arrive 11 minutes late. You provide 47 minutes of psychotherapy. The correct code is 90834, not 90837, because the psychotherapy time was 47 minutes, not 60.
Another version: the patient is present for 58 minutes, but 9 minutes of that was documentation at the end of the session. The psychotherapy time is 49 minutes. Again, 90834.
The appointment slot is not the billing unit. The direct psychotherapy time is.
What your 90837 note must document to survive an audit
Once you know the correct code, your note has to prove it. CMS requires time documentation for 90832, 90834, and 90837, specifically, start/stop time or total psychotherapy time. (CMS)
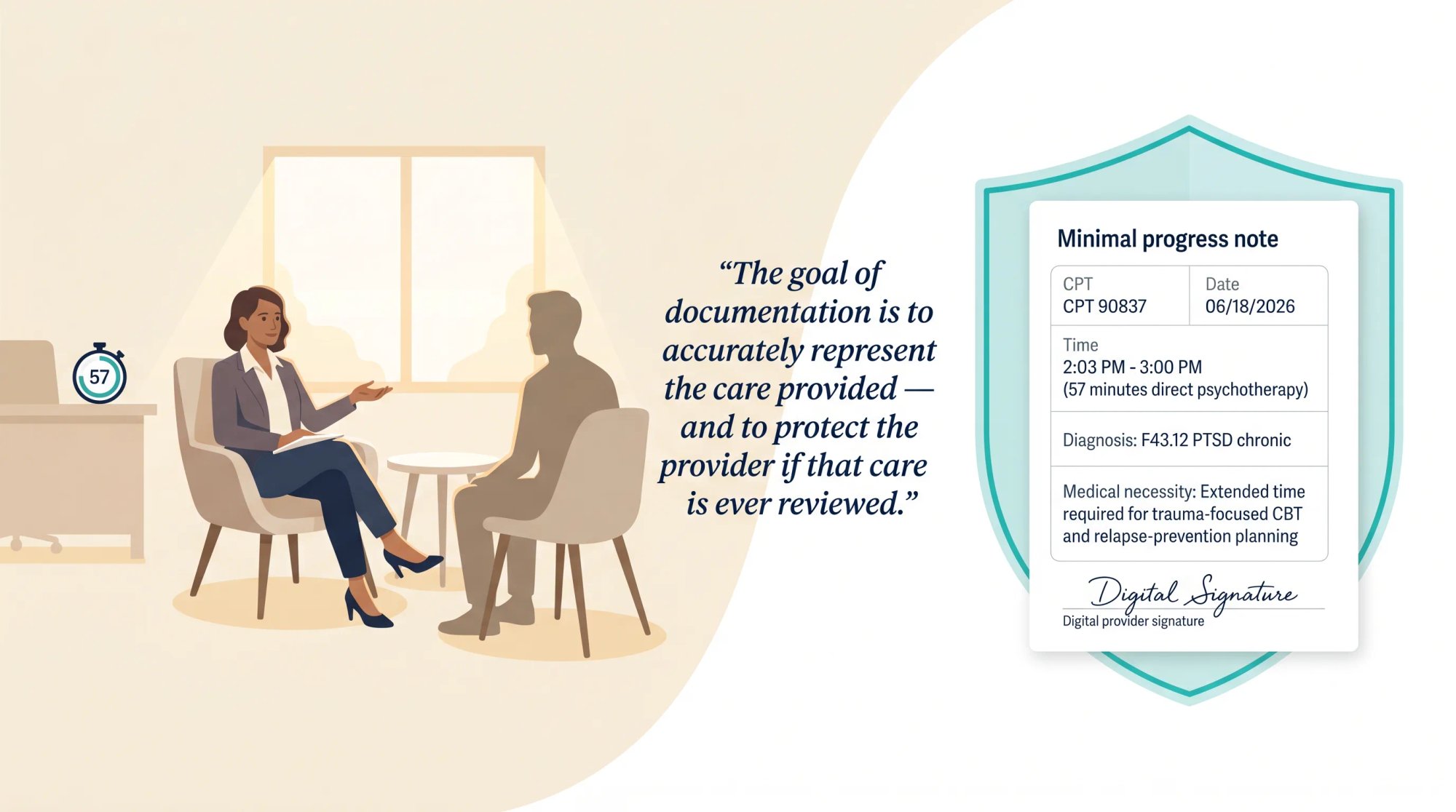
Start/stop time is the stronger option. It is harder to attack in an audit because it creates a specific, time-stamped record. Total time is acceptable but allows more room for challenge, a note that says "60-minute session" is not the same as one that says "Total psychotherapy time: 57 minutes," and neither is as solid as one that says "2:03 PM – 3:00 PM; 57 minutes direct psychotherapy."
Elements of an audit-ready 90837 progress note
CGS Medicare's post-payment review checklist for psychotherapy services asks reviewers to look for: the date of service, time spent, a note supporting face-to-face service, a treatment plan, the diagnosis, symptoms, functional status, mental status, progress, prognosis, and provider signature with credentials. (CGS Medicare)
In practice, an audit-ready 90837 note includes all of these:
| Element | What to document |
|---|---|
| Patient identity | Name or patient ID |
| Date of service | Exact date |
| Provider | Name, credential, signature |
| Code | 90837 |
| Time | Start/stop or total direct psychotherapy time |
| Modality | In person, audio-video telehealth, audio-only if allowed |
| Patient presence | Patient present; note anyone else who joined |
| Diagnosis | ICD-10-CM code at highest specificity |
| Symptoms | Current presentation and severity |
| Functional impairment | How symptoms affect work, school, relationships, safety, daily functioning |
| Risk/safety | Suicide/self-harm/SUD relapse risk as clinically relevant |
| Mental status | As clinically appropriate |
| Intervention | Specific psychotherapy methods used, not generic labels |
| Patient response | Engagement, insight, progress, barriers |
| Medical necessity for 90837 | Why 53+ minutes was needed on this date |
| Plan | Next steps, frequency, homework, referrals, safety plan |
| Treatment-plan link | How the session connects to active treatment goals |
The note that survives audit versus the note that doesn't
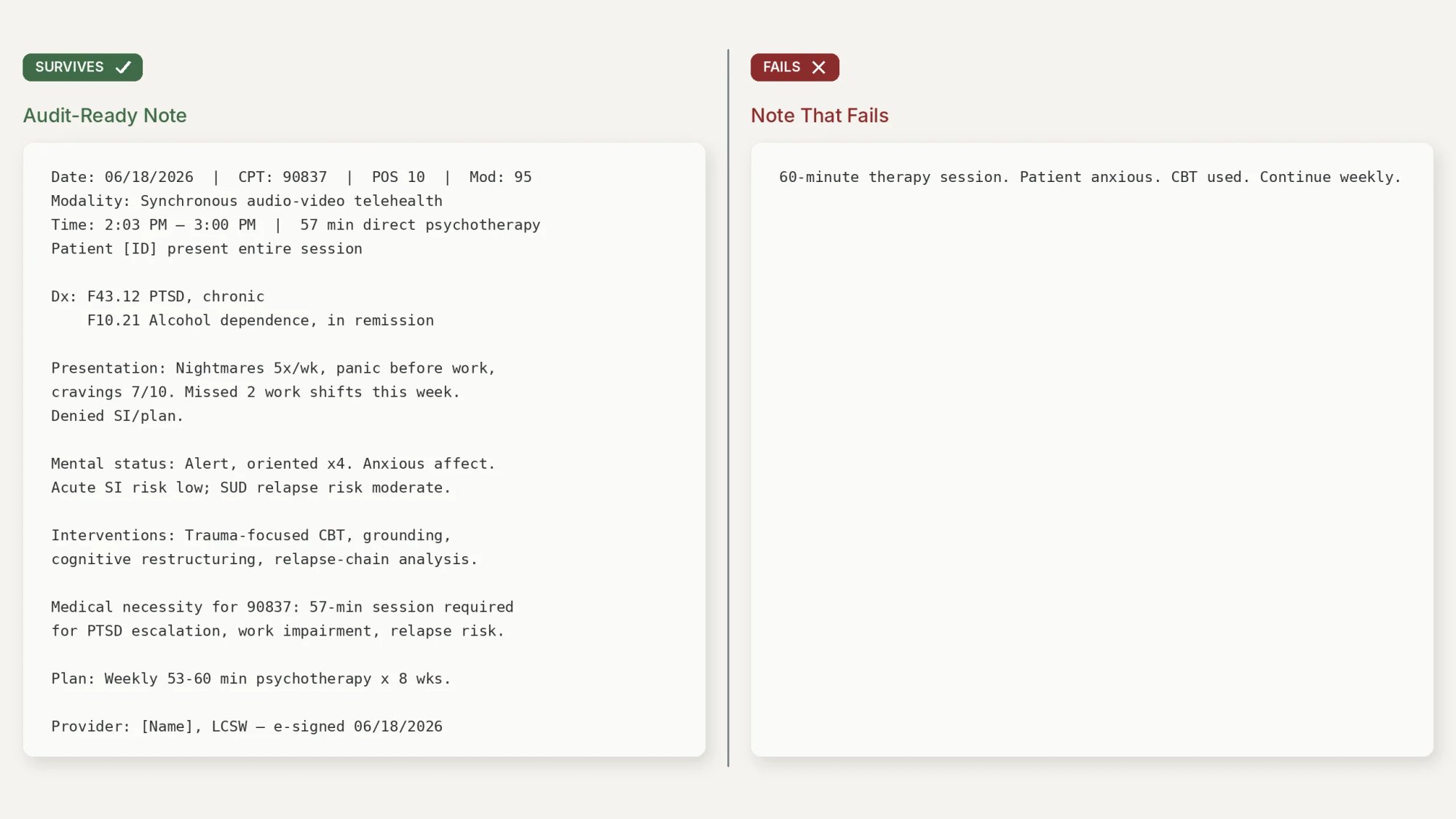
Here is a documentation example that would survive scrutiny:
Date of service: 06/18/2026
CPT/POS/modifier: 90837, POS 10, modifier 95
Modality: Synchronous audio-video telehealth
Patient location: Patient at home in Austin, Texas
Provider location: Provider office in Texas
Consent: Telehealth consent confirmed
Time: 2:03 PM - 3:00 PM; 57 minutes direct psychotherapy.
Participants: Patient present for entire session. Spouse joined 2:43-2:51 PM
with patient consent for safety-plan support.
Diagnosis:
F43.12 Post-traumatic stress disorder, chronic
F10.21 Alcohol dependence, in remission
Presentation:
Patient reported nightmares 5 nights/week, panic before work, increased
avoidance, and cravings rated 7/10 after conflict with spouse. Missed two
work shifts this week. Denied current suicidal intent or plan.
Mental status/risk:
Alert and oriented x4. Mood anxious; affect constricted. Thought process
linear. No psychosis observed. Acute suicide risk low today; relapse risk
moderate due to cravings and avoidance.
Interventions:
Provided trauma-focused CBT, grounding practice, cognitive restructuring
around trauma-related avoidance, relapse-chain analysis, and rehearsal of
coping responses for evening cravings. Spouse joined briefly to review
agreed support steps and removal of alcohol cues from home.
Response:
Patient initially tearful and avoidant but completed grounding exercise
and identified three high-risk relapse triggers. Patient agreed to use
written coping plan and contact sponsor if cravings exceed 8/10.
Medical necessity for 90837:
A 57-minute session was medically necessary due to PTSD symptom escalation,
work impairment, and increased SUD relapse risk. Extended time was required
to complete trauma-focused processing, stabilize anxiety with grounding,
and create a relapse-prevention plan before session termination.
Plan:
Continue weekly 53-60 minute individual psychotherapy for 8 weeks, then
reassess. Homework: daily grounding practice, craving log, sponsor contact
plan. Patient instructed to use crisis plan if suicidal intent develops.
Provider signature:
Jane Doe, LCSW
Electronically signed 06/18/2026
And here is the note that fails, and still gets submitted daily:
60-minute therapy session. Patient anxious. CBT used. Continue weekly.
That note does not prove 53+ minutes of psychotherapy. "60-minute session" could mean the appointment block, not the direct therapy time. There is no start/stop time, no ICD-10-CM specificity, no functional impairment, no clinical rationale for why 90837 rather than 90834 was appropriate. It would not survive an ADR (Additional Documentation Request, the payer's post-payment request for records). This is the kind of note that can lose in an audit even when the clinician actually did the work. (CGS Medicare)
Time documentation is the first thing an auditor checks. But it is not the only thing. Documenting that the session lasted 53+ minutes is different from documenting that it needed to.
How to document medical necessity for a 90837 session
This is the part of 90837 billing that most practices underestimate. A payer can deny 90837 even when the time is correctly documented, if the note does not explain why this patient, on this date, required 53 or more minutes of psychotherapy rather than a shorter session.
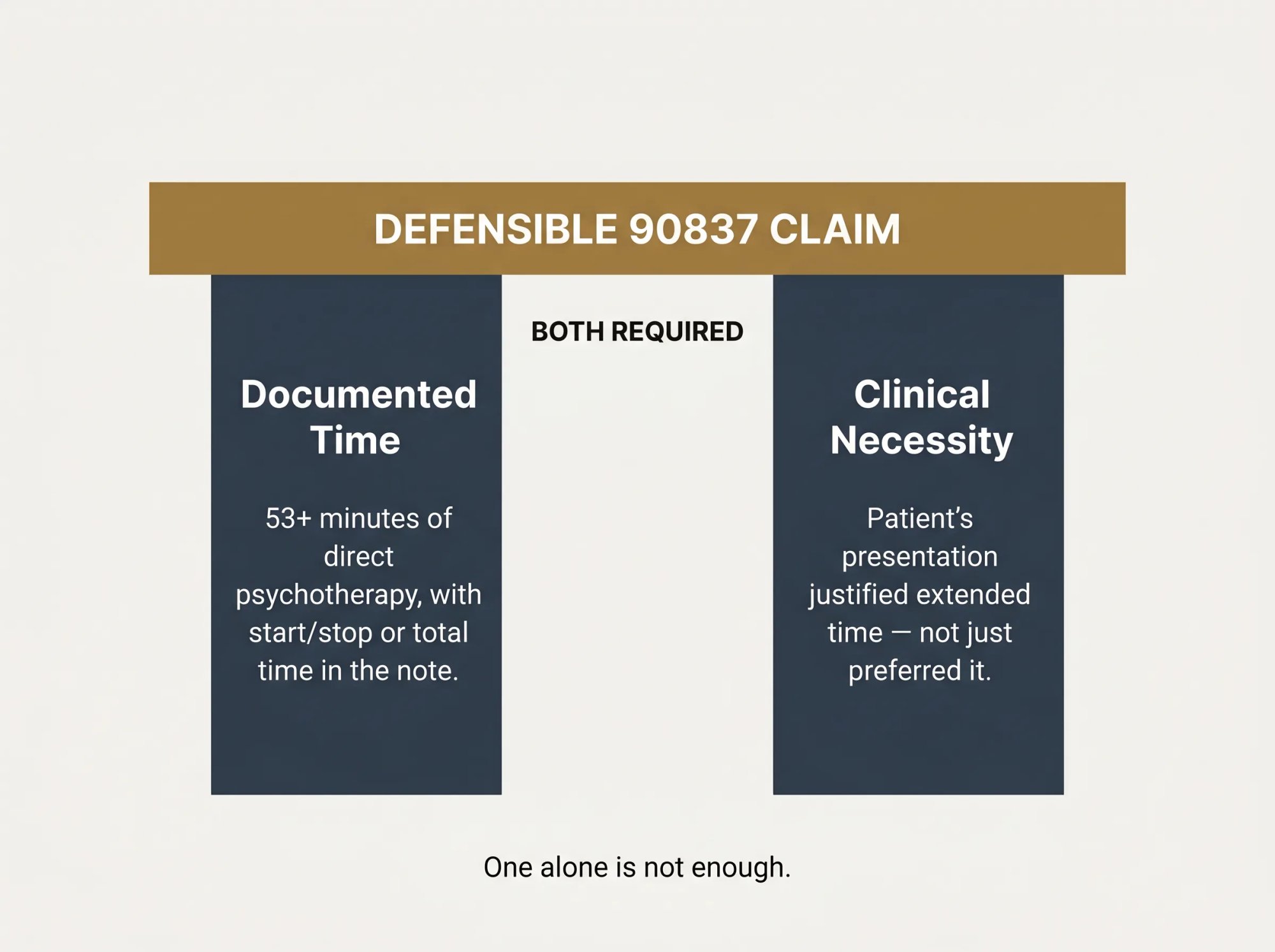
There are two requirements that must both be true for a defensible 90837:
- The session actually included at least 53 minutes of direct psychotherapy.
- The patient's clinical presentation justified that amount of psychotherapy time.
Meeting only the first requirement is not enough.
What clinically justifies 90837 extended session time
Strong clinical reasons that can support 90837, when the note is specific to the patient and the date:
- Severe depression with functional impairment requiring extended CBT, behavioral activation, safety assessment, and coping-plan work
- PTSD or complex trauma requiring trauma-focused processing, stabilization, grounding, or exposure work that cannot be safely abbreviated
- OCD requiring exposure and response prevention that has a minimum effective length
- Substance use disorder relapse-prevention work involving craving triggers, relapse-chain analysis, recovery planning, and co-occurring psychiatric symptoms
- Recent inpatient hospitalization or discharge transition requiring stability assessment and crisis planning
- Active suicidal ideation, self-harm risk, or acute safety planning need
- Bipolar disorder, psychosis, or severe anxiety presentations requiring extended stabilization
- Significant functional impairment affecting work, school, relationships, or daily living that requires multi-component clinical work within a single session
- Family or caregiver involvement needed during an individual session to address safety, relapse risk, communication barriers, or treatment-plan implementation
What does not justify billing 90837
These reasons are not sufficient on their own:
- "Patient prefers 60-minute sessions"
- "My standard session length is 60 minutes"
- "Insurance reimburses more for 90837"
- "Patient was talkative"
- "Rapport building"
- "Ongoing anxiety and depression" with no severity, impairment, intervention detail, or rationale for the extended duration
The problem with that last one is subtle and important. A diagnosis of "ongoing anxiety" or "ongoing depression" is a legitimate diagnosis. But a note that lists the diagnosis without specifying current severity, functional impact, the specific clinical work done during the extended time, and why shorter wouldn't have served the patient. That note does not support 90837. It supports a psychotherapy visit. It doesn't support this length of psychotherapy visit.
How to write a medical necessity rationale for 90837
The note should include one or two patient-specific sentences that directly answer: why 53+ minutes, today? Examples of how this reads in practice:
Medical necessity for 90837: Extended psychotherapy time was required today due to increased panic symptoms, avoidance behavior, and work impairment. The session required prolonged CBT exposure planning, cognitive restructuring, and grounding practice to stabilize symptoms before session termination.
Medical necessity for 90837: Patient presented with increased cravings and recent high-risk relapse triggers. A 57-minute session was necessary to complete relapse-chain analysis, motivational interviewing, coping-skills rehearsal, and a written relapse-prevention plan.
Why your treatment plan is as important as your session note
For providers who bill 90837 regularly, the treatment plan is as important as the session note. CGS Medicare's documentation guidance specifically expects an individualized treatment plan showing the type, amount, frequency, duration, diagnoses, goals, and expectation of improvement or deterioration if treatment is withdrawn. (CGS Medicare)
A treatment plan that simply lists the diagnosis and "weekly psychotherapy" is not enough. A treatment plan that says "weekly individual CBT/DBT-informed psychotherapy, 53-60 minutes, for 12 weeks, with reassessment every 4 sessions", and includes measurable goals tied to specific symptoms, is the documentation foundation that makes every weekly 90837 defensible as a pattern, not just individually.
The notes we review most often in pre-audit preparation are ones where the clinician clearly did 60 minutes of meaningful clinical work, but the note never explains why that patient, on that day, couldn't have been adequately served in 45 minutes. That one missing sentence is the difference between a clean claim and an ADR.
Medical necessity and time documentation protect your individual claims. But payers also look at patterns across claims, and that's where the next layer of risk lives.
Why 90837 gets audited, and what the OIG actually found
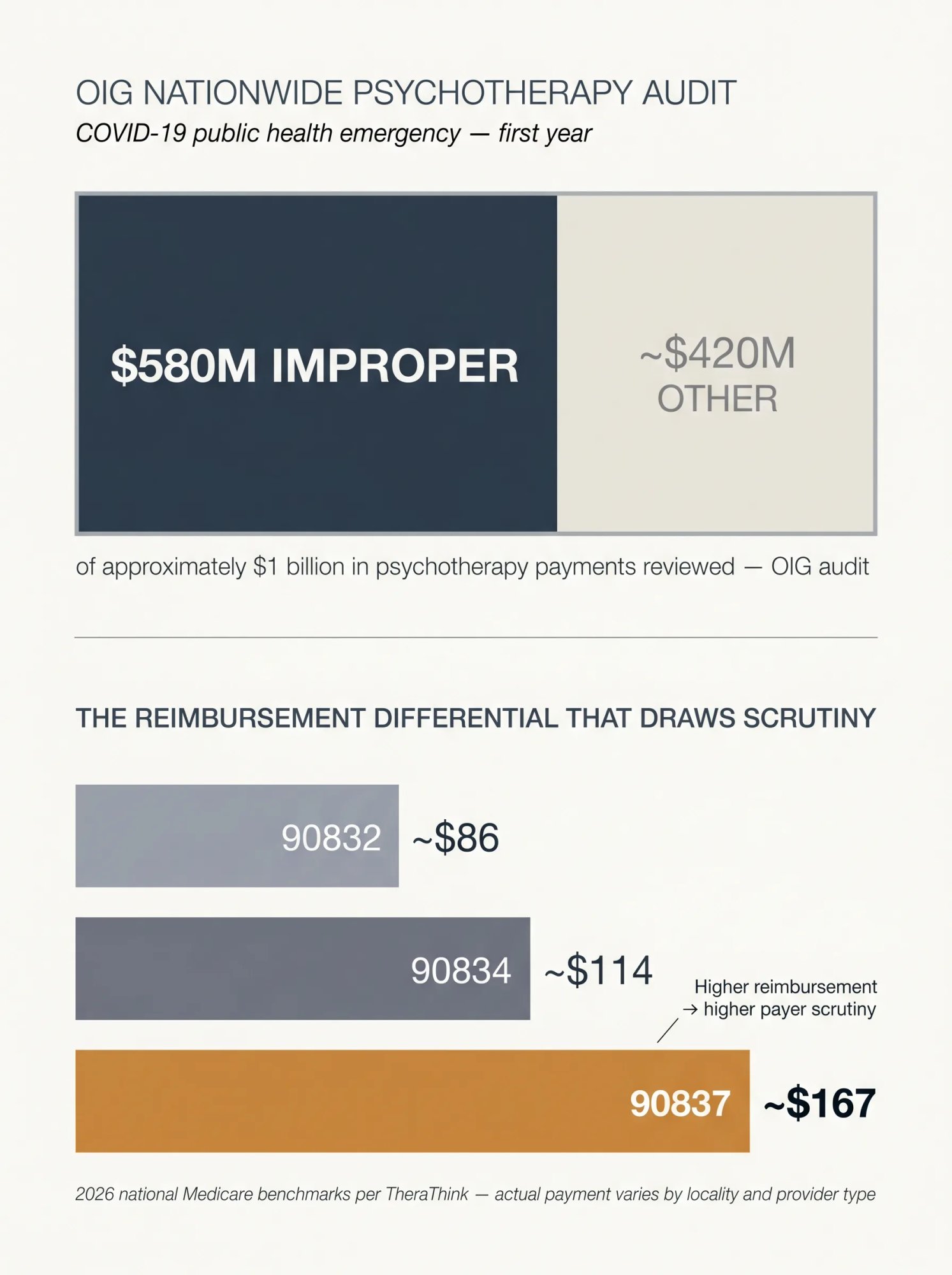
CPT 90837 pays more than 90834. That differential is meaningful: a 2026 national Medicare benchmark lists 90837 at approximately $167, compared to roughly $114 for 90834 and $86 for 90832, according to behavioral-health reimbursement tracking data from TheraThink. (TheraThink) Payers track utilization distributions, and a provider who bills 90837 significantly more often than peer comparators will attract attention, not because the code is banned, but because the pattern raises a question: does every session genuinely need 60-minute-level time?
Medicare's audit history for 90837, what CGS and OIG found
In 2021, CGS Medicare announced post-payment review targeting CPT 90832, 90834, and 90837 after CMS directed Medicare Administrative Contractors to resume medical reviews. CGS stated that providers were selected based on high error rates, potential overutilization, and comparative billing analysis, and that the review would check whether services were medically necessary, correctly coded, and delivered as billed. Providers receiving an ADR had 45 days to submit documentation. Failure to respond or failure to document the service adequately could result in denial and recoupment. (CGS Medicare)
That's not a hypothetical. The OIG conducted a nationwide audit of psychotherapy services during the COVID-19 public health emergency's first year and estimated $580 million in improper payments out of approximately $1 billion in total psychotherapy payments reviewed, with failures including missing psychotherapy time documentation, missing provider signatures, and services that did not meet Medicare requirements. (OIG HHS)
In a separate audit of a New York City provider with high psychotherapy billing, OIG found that every sampled beneficiary day failed at least one Medicare requirement. The specific failures: missing treatment plans, missing frequency and duration elements, incident-to supervision issues, missing psychotherapy time documentation, and notes that lacked physician signatures. OIG estimated approximately $1.1 million in overpayments from that single provider review. (OIG HHS)
How commercial payers scrutinize 90837 utilization
Medicare is not alone. Commercial payers have sent utilization letters to clinicians whose 90837 use was materially higher than peer billing distributions. Around 2017, provider-association and practice-management reports described utilization letters about high 90837 use from or on behalf of Anthem and Medical Mutual of Ohio, with Highmark also reported. These examples illustrate the kind of payer scrutiny that remains relevant, though they reflect historical secondary reporting rather than current official payer policies. (CarePaths)
An important note on a recent development: in June 2026, APA Services and the American Psychiatric Association urged Aetna to pause reimbursement reductions affecting Alma-affiliated clinicians, including reimbursing CPT 90837 at the same rate as 90834. (Becker's Payer Issues) This is a specific situation involving a particular clinician network and contracting terms. It does not represent general Aetna policy for all plans and all providers. But it illustrates that commercial reimbursement for 90837 is under payer scrutiny in multiple forms simultaneously.
The billing pattern that triggers 90837 audits
Billing 90837 every week is not automatically wrong. Billing 90837 every week with thin, cloned, or time-deficient notes is exactly what payers look for.
We help practices run internal utilization reviews before an ADR arrives. If your 90837 rate across your caseload is significantly higher than your 90834 rate, without treatment plans and notes that clinically justify extended sessions for each patient. That is the pattern that attracts scrutiny. The solution is not to avoid 90837. It is to make sure every 90837 you bill is backed by documentation that can withstand review.
Beyond utilization patterns, there is a coding trap that catches many behavioral health providers who do both therapy and medication management.
Add-on psychotherapy codes: when 90837 is not the right code
The E/M plus psychotherapy rule, 90837 vs 90838
When a psychiatrist, psychiatric nurse practitioner, or other qualified prescriber provides a separately identifiable E/M service (medication management, medical evaluation) and also provides individual psychotherapy on the same date, the billing is not the standalone 90837.
The correct approach:
- Bill the appropriate E/M code for the medication management portion
- Bill the psychotherapy add-on code for the psychotherapy portion
- Use +90838 when the psychotherapy portion alone is 53 or more minutes
The result for a session with medication evaluation plus 54 minutes of separately identifiable psychotherapy is: 99214 + 90838, not 99214 + 90837.
That distinction matters because 90837 is a standalone code, not an add-on. Billing it alongside an E/M code is a coding error, and it is one that CMS guidance is explicit about: the E/M time does not count toward the psychotherapy add-on time, and the add-on code is what is used when psychotherapy is performed with an E/M service. (CMS)
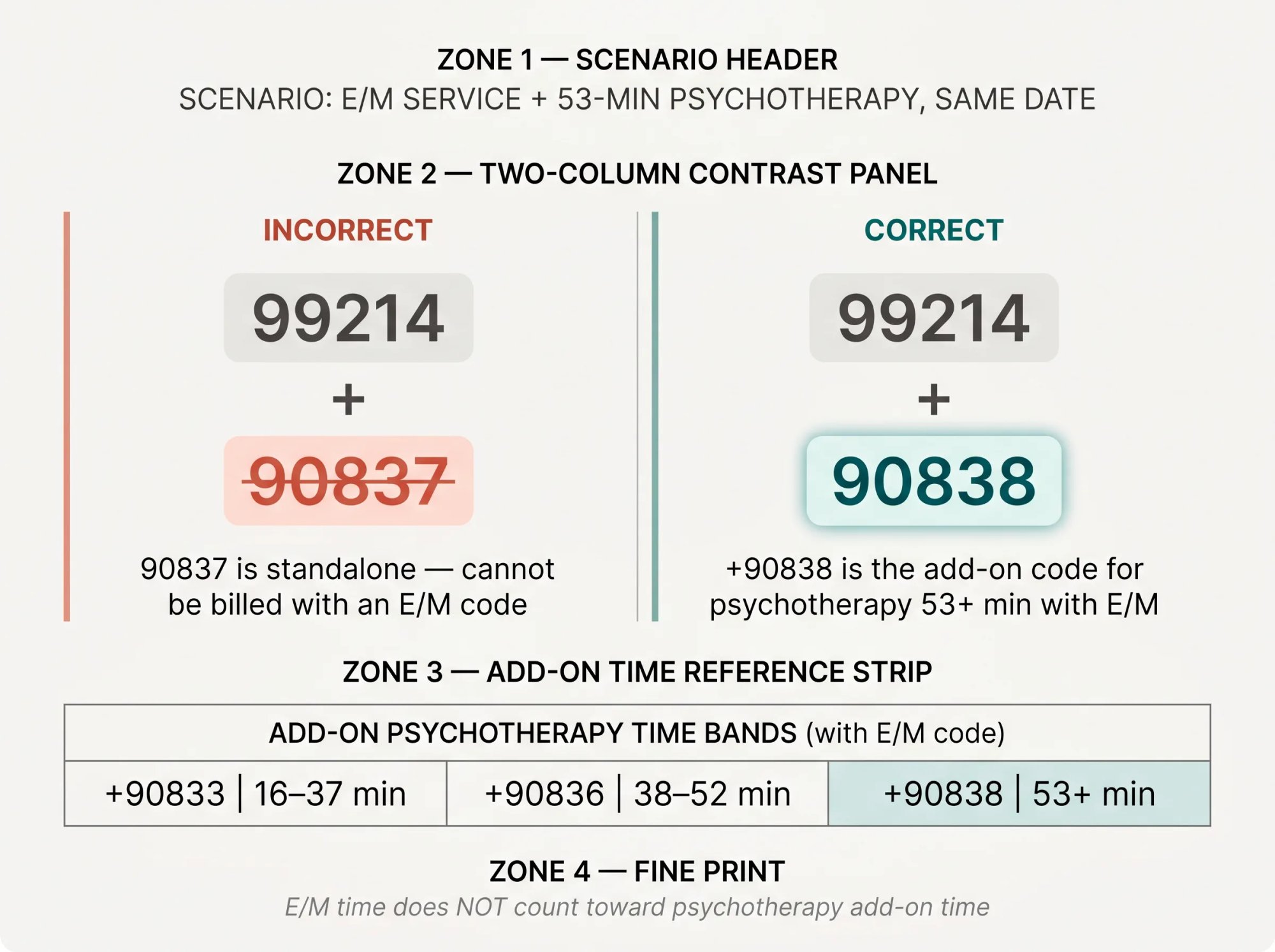
The full add-on psychotherapy codes, used with E/M visits:
| Add-on | Used with | Time |
|---|---|---|
| +90833 | E/M code | 16-37 minutes |
| +90836 | E/M code | 38-52 minutes |
| +90838 | E/M code | 53+ minutes |
When to add +90785 for interactive complexity
CPT +90785 is an add-on code for interactive complexity. It is not a time-extension code and not a "difficult session" code. It reflects specific communication factors that make psychotherapy more complex to deliver.
CMS says 90785 may be reported with 90832, 90834, 90837, and the psychotherapy add-on codes 90833, 90836, and 90838. It may also be reported with psychiatric diagnostic evaluation codes. It should not be billed when the patient cannot communicate by any means. (CMS)
The qualifying communication factors include situations involving legal guardians, family members, interpreters or translators, child welfare agencies, parole or probation officers, schools, or other third parties. CMS describes interactive complexity as appropriate when at least one qualifying communication difficulty exists – such as maladaptive communication, caregiver emotions or behaviors interfering with treatment, mandated reporting or sentinel events, or the use of play equipment, physical devices, or interpreters to overcome significant communication barriers. (CMS)
What this looks like in a defensible note:
90837 + 90785
Patient is a 9-year-old with PTSD. Session required use of play materials
and repeated caregiver redirection because caregiver's emotional responses
interfered with treatment-plan implementation. Clinician spent 12 minutes
managing interactive complexity while maintaining therapeutic engagement.
What this does not look like:
Patient was difficult.
That is not enough to support 90785. Interactive complexity requires documentation of the specific qualifying communication factor, not a general description of session difficulty.
Telehealth modifiers and place of service codes for 90837
Modifier selection for 90837 telehealth claims is one of the most payer-variable parts of behavioral health billing. Do not assume that a modifier that applies to Medicare fee-for-service will apply to a commercial plan, a Medicaid managed care plan, or a Medicare Advantage plan with the same network.
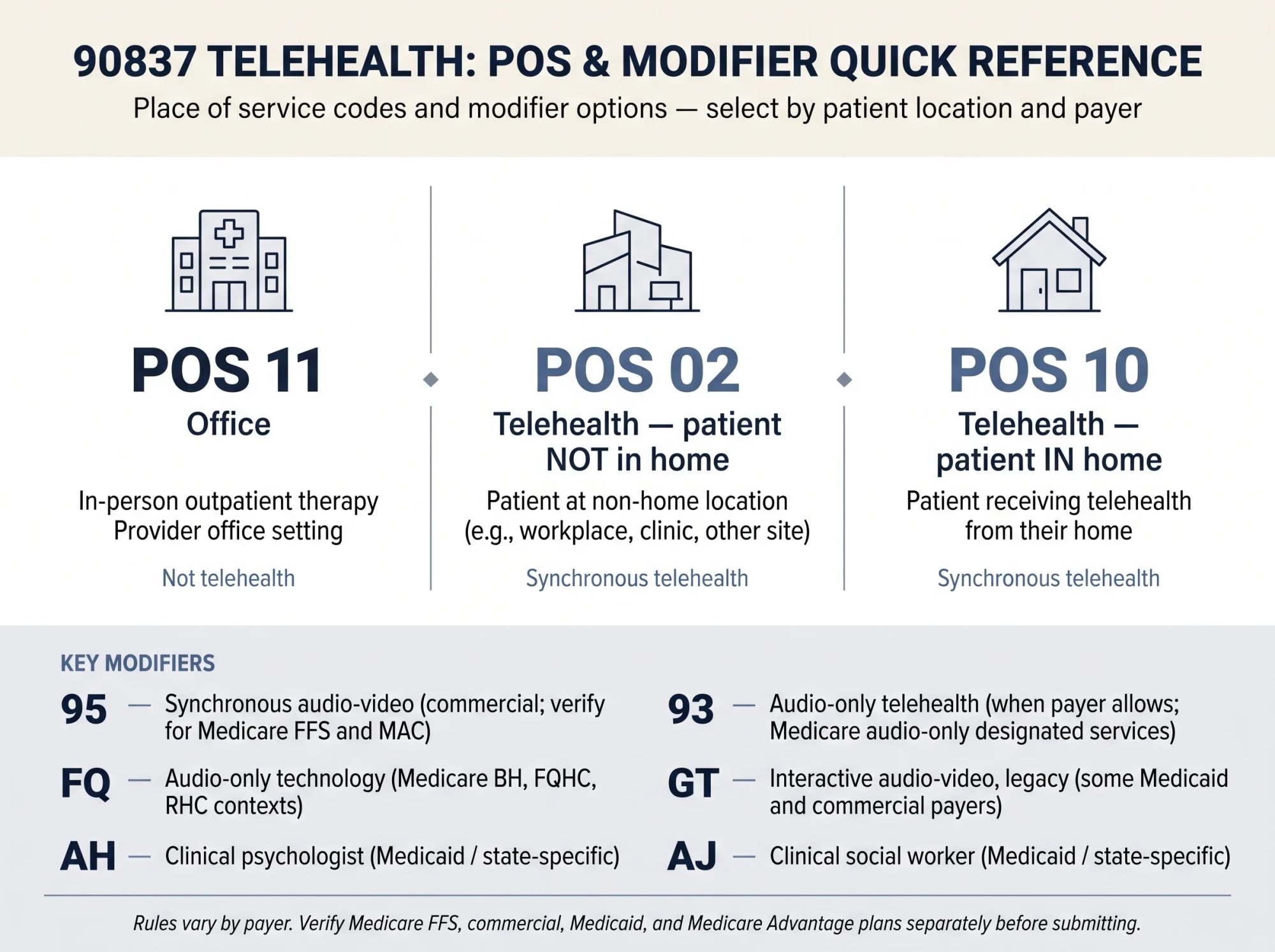
Modifier options for telehealth 90837 claims
| Modifier | Common meaning | When it applies |
|---|---|---|
| 95 | Synchronous audio-video telehealth | Common for commercial synchronous audio-video telehealth; Medicare FFS use is more limited and MAC-specific, verify payer or MAC policy |
| 93 | Audio-only telehealth | Used when the payer allows audio-only; Medicare references 93 for audio-only designated services |
| FQ | Audio-only communication technology | Used in certain Medicare behavioral-health, FQHC, and RHC contexts |
| GT | Interactive audio-video (legacy) | Still required by some Medicaid and commercial payers; Noridian requires GT for CAH Method II institutional claims |
| 25 | Significant, separately identifiable E/M | Sometimes required on the E/M code when billed alongside a psychotherapy add-on; not a universal default |
| AH | Clinical psychologist | Often Medicaid- or state-specific |
| AJ | Clinical social worker | Often Medicaid- or state-specific |
| HO/HN | Master's/bachelor's level provider | Common in Medicaid behavioral health programs |
Telehealth billing errors commonly involve the wrong code, the wrong modality modifier, the wrong place of service code, or insufficient documentation of the telehealth encounter. (HHS Telehealth)
Place of service codes for 90837 telehealth visits
| POS | Meaning | When to use |
|---|---|---|
| 11 | Office | In-person outpatient therapy in office |
| 02 | Telehealth, patient not in home | Patient receives telehealth from a non-home location |
| 10 | Telehealth, patient in home | Patient receives telehealth from home |
| 12 | Home | In-person service in patient's home |
| 22 | Outpatient hospital | Hospital outpatient behavioral health |
Noridian confirms: POS 02 is for telehealth when the patient is not in the home; POS 10 is for telehealth when the patient is in the home; and modifier 93 is used for audio-only services when the code is designated as audio-only eligible. Providers must be licensed and enrolled in the state where the service is furnished. (Noridian Medicare)
Permanent Medicare telehealth rules for behavioral health
As of HHS's February 2026 policy update, several telehealth flexibilities are now permanent or extended for Medicare behavioral and mental health services: (HHS Telehealth)
- Medicare patients can receive behavioral and mental health telehealth services from home permanently
- Geographic restrictions for behavioral and mental health telehealth are permanently removed
- Audio-only behavioral and mental health telehealth is permanently available when allowed conditions are met
- The in-person visit requirement for behavioral and mental health telehealth is waived through December 31, 2027
- Marriage and family therapists and mental health counselors are permanent Medicare distant-site providers
For audio-only, CMS guidance states that Medicare can allow audio-only for behavioral and mental health services when the provider is technically capable of audio-video and the patient cannot use, does not wish to use, or does not consent to video. (CMS)
Telehealth documentation checklist for 90837
Include in the note:
Modality: audio-video or audio-only
Patient location: exact state and setting (e.g., patient's home in Florida)
Provider location: state and setting
Consent: telehealth consent confirmed
Time: start/stop or total psychotherapy time
Audio-only reason, if applicable: patient preference, technology limitation,
inability to use video, patient preference not to use video, etc.
For commercial payers and Medicaid, do not assume Medicare rules apply. Telehealth coverage, modifier requirements, POS codes, audio-only allowance, and state licensure rules all vary.
Does 90837 require prior authorization?
There is no single national answer to "does 90837 require prior authorization?" The answer depends on the payer, the specific plan product, the state, the network, the employer group benefit design, and whether the behavioral health benefit is managed by a carve-out vendor rather than the primary plan.
This matters enormously in behavioral health. The insurer whose card the patient presents – Aetna, UnitedHealthcare, Cigna, may not be the entity managing the behavioral health benefit. Behavioral health benefits are frequently carved out to managed behavioral health organizations such as Optum/United Behavioral Health, Carelon, Evernorth, or Magellan. If you submit a claim to the medical plan without recognizing the carve-out, you are billing the wrong payer, and the claim will fail regardless of how strong your documentation is.
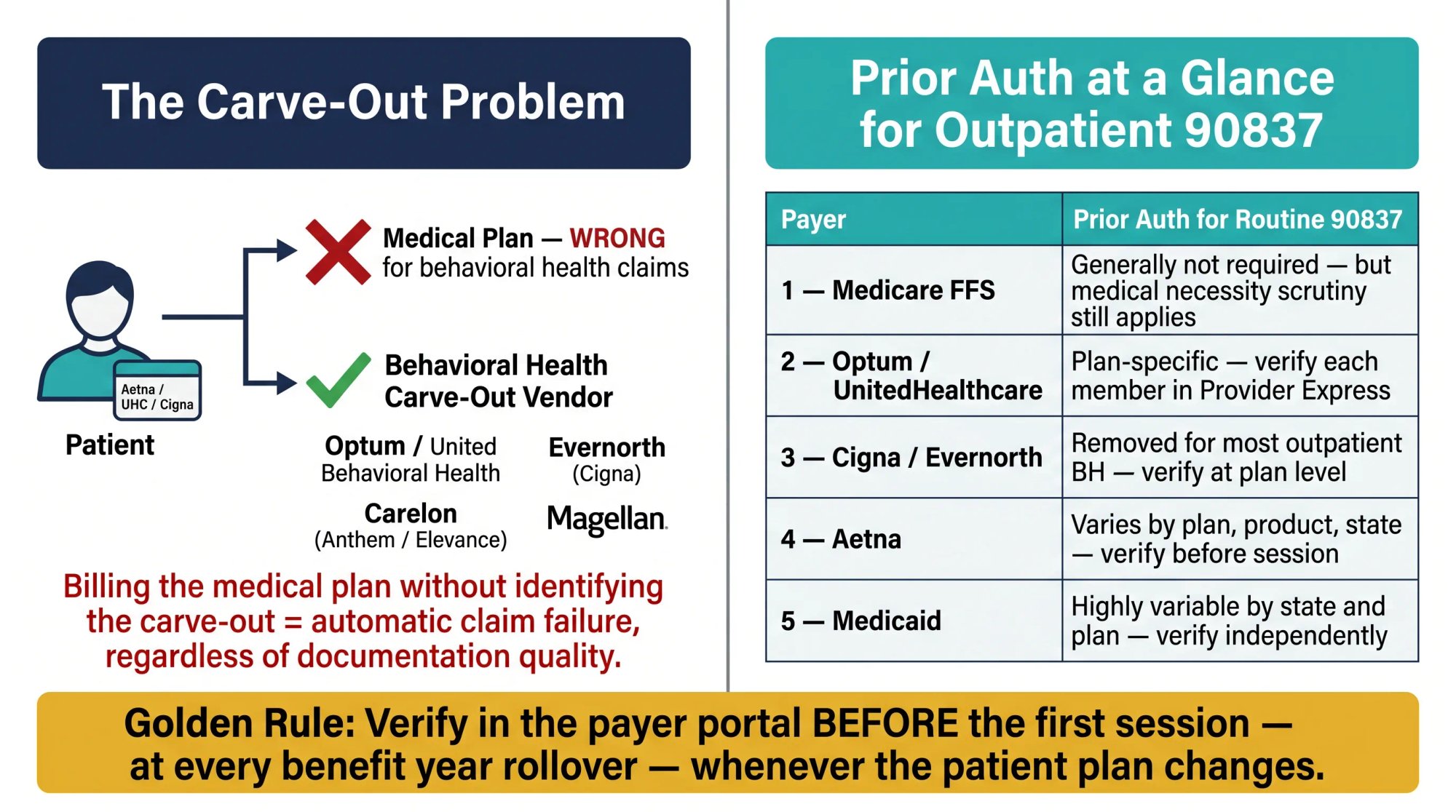
Prior authorization requirements by payer
Medicare fee-for-service: Traditional Medicare generally does not require routine prior authorization for ordinary outpatient psychotherapy. However, claims remain subject to medical necessity documentation requirements, LCD and CMS billing article rules, post-payment review, audits, and MUE edits. No prior auth does not mean no scrutiny.
Optum / UnitedHealthcare: Optum-administered plans may require authorization or notification for specialty outpatient services and most inpatient services, but authorization rules are plan-specific. For routine outpatient 90837, verify the member's specific benefits and authorization requirements in Provider Express rather than assuming the specialty-outpatient category applies. Notably, UnitedHealthcare's Gold Card program can waive prior authorization for eligible behavioral health procedure codes for eligible providers and plans, but Gold Card eligibility is provider-specific and plan-specific. (Optum Provider Express) UHC's Exchange plan authorization lists are published by state, and prior auth requirements differ across products. (Provider Express)
Cigna / Evernorth: Evernorth has stated publicly that it removed prior authorization from most behavioral health treatments and that routine outpatient mental health and substance use disorder care does not require prior authorization under its plans, while acknowledging that rare treatments may still require it. (Cigna Group Newsroom) Verify at the plan level, not all Cigna-branded products are administered by Evernorth.
Aetna: Aetna's requirements depend on the member's plan, product, network, and state. Aetna offers retrospective review – a post-treatment coverage process based on eligibility, benefits, clinical data, and documentation, but only in limited circumstances. It is generally not a substitute for missed required precertification, and state requirements may supersede Aetna's standard rules. (Aetna)
Medicaid and managed Medicaid: Medicaid is the most variable of all. Some state fee-for-service Medicaid programs cover 90837 without authorization. Others require authorization after a set number of visits. Many Medicaid programs carve behavioral health out to a managed care vendor. Associate-level provider coverage, session limits, diagnosis restrictions, and visit frequency rules vary by state and plan. Treat every Medicaid plan as a separate verification task.
The most important rule in prior authorization management for behavioral health: verify in the payer portal before the first session, at every benefit year rollover, and whenever a patient's plan changes. Checking eligibility on the medical plan does not tell you whether the behavioral benefit has different auth rules through a carve-out vendor.
What Medicare and commercial payers pay for 90837
Understanding how 90837 is reimbursed helps you evaluate whether claims are paying correctly and what is at stake when a claim is denied.
Medicare payment methodology
Medicare does not pay one flat national rate for every provider in every location. CMS's physician fee schedule calculates payment based on relative value units (RVUs), a conversion factor, and geographic practice cost indices (GPCIs) that adjust for local costs. The CY2026 final rule established conversion factors of $33.57 for qualifying APM participants and $33.40 for nonqualifying APM participants. (CMS) CMS's physician fee schedule lookup tool is the official source for rate verification by locality and provider type. (CMS)
For rate context: a behavioral-health reimbursement tracker lists 2026 Medicare national benchmarks at approximately $167 for CPT 90837, $114 for 90834, and $86 for 90832. (TheraThink) These are national benchmark figures, not a payment guarantee. Actual Medicare payment varies by locality, facility or non-facility setting, provider type and payment rules (clinical social workers, MFTs, and mental health counselors are paid at 75% of the clinical psychologist physician fee schedule amount for certain services), and fee schedule methodology. (CMS)
Commercial reimbursement
Commercial rates vary substantially by payer, state, product, network, and individual contract. PayerPrice's June 2026 aggregation of payer price-transparency file data lists national average in-network benchmarks for 90837 as approximately:
| Payer | National average (90837) |
|---|---|
| Blue Cross Blue Shield | ~$158 |
| UnitedHealthcare | ~$139 |
| Aetna | ~$146 |
| Cigna | ~$196 |
Source: (PayerPrice) These are aggregator-derived transparency-file averages, not official payer fee schedules or expected contract rates – actual commercial reimbursement depends on the specific payer, product, locality, network, and contract.
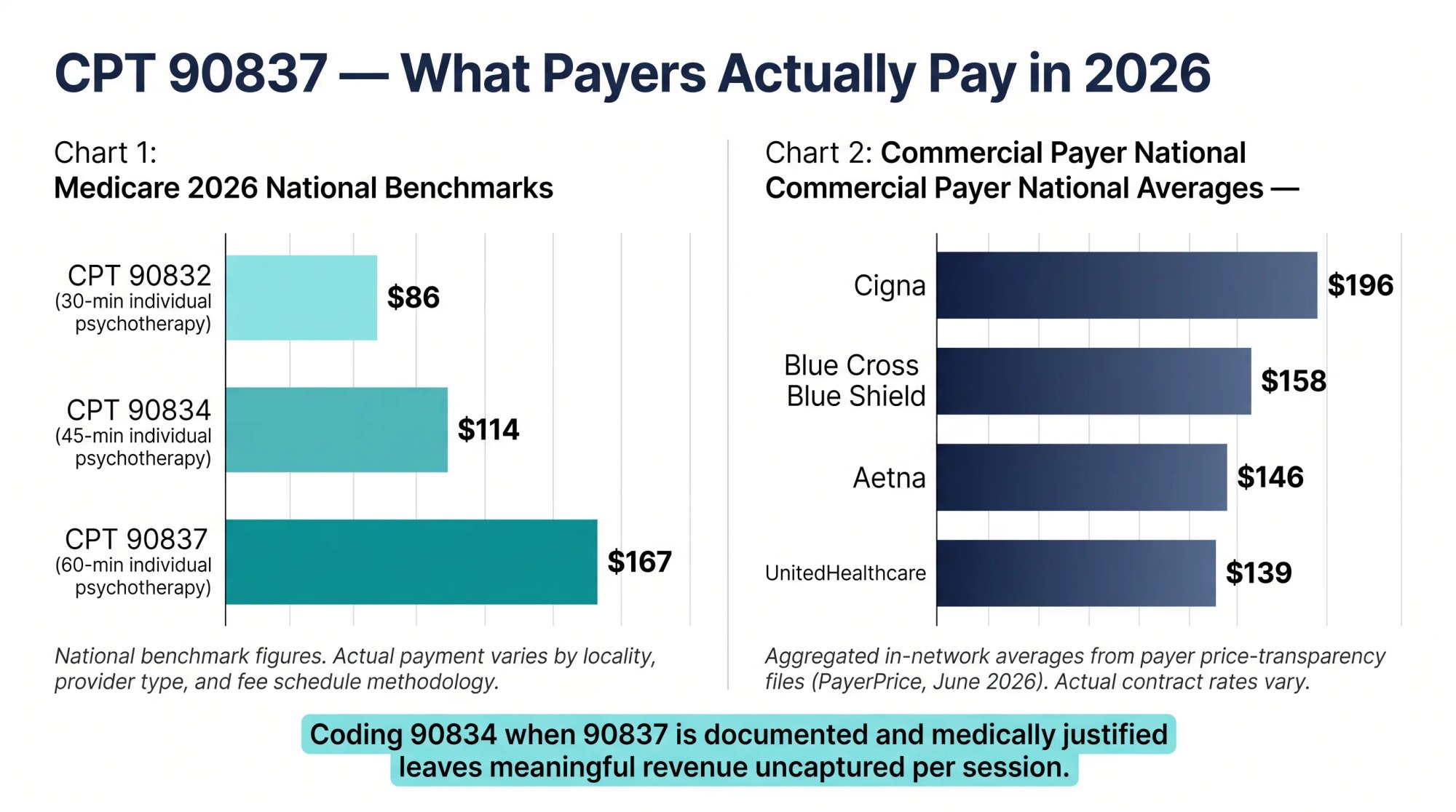
The rate differential between 90837 and 90834 across all payers illustrates why correct code selection matters beyond compliance: accurately coding a 57-minute session as 90837 instead of defaulting to 90834 reflects real, properly earned revenue. Failing to bill 90837 when the time and medical necessity are documented is as much a problem as billing 90837 when they are not.
Common reasons 90837 gets denied, and how to appeal
90837 denial reasons and how to prevent each one
| Denial reason | Why it happens | How to prevent it |
|---|---|---|
| Missing time | Note says "60-minute session" but no actual psychotherapy time documented | Document start/stop or total direct psychotherapy time |
| Wrong time band | 50-52 minutes billed as 90837 | Bill 90834 unless documented psychotherapy time is 53+ |
| Scheduled time used | Appointment was 60 minutes but therapy was shorter | Code actual psychotherapy time, not appointment slot |
| Medical necessity not supported | Note doesn't explain why 53+ minutes was needed | Add patient-specific rationale tied to symptoms, impairment, and interventions |
| Generic notes | Same note language session after session | Document session-specific symptoms, interventions, patient response, and plan |
| High utilization | Provider bills 90837 for nearly every patient | Ensure treatment plans and notes justify frequency and duration per patient |
| Missing treatment plan | No individualized goals, frequency, duration, diagnosis, progress | Maintain active individualized treatment plans for each patient |
| Diagnosis problem | Unspecified or unsupported ICD-10-CM | Code diagnosis to highest specificity supported by the record |
| Signature problem | Missing provider signature or credentials | Sign every note with credential and date |
| E/M coding error | 90837 billed alongside E/M code | Use E/M + 90838 when psychotherapy portion is 53+ with E/M service |
| Interactive complexity error | 90785 added without meeting criteria | Document qualifying communication difficulty and time |
| Crisis-code conflict | 90837 billed with 90839 or 90840 | Use correct code family; don't combine routine and crisis psychotherapy codes |
| Telehealth POS/modifier error | Wrong POS 02/10 or missing/wrong modifier | Follow payer-specific telehealth billing rules |
| Audio-only not covered | Payer doesn't cover audio-only or wrong modifier used | Verify plan coverage and document audio-only reason |
| Authorization missing | Plan required auth/notification before service | Check portal before service for every new patient and benefit period |
| Duplicate/MUE denial | Multiple units same day | Verify MUE limits; avoid routine multiple units without explicit payer guidance (CMS MUE) |
| Incident-to/supervision issue | Rendering provider not qualified or required supervision was absent | Follow payer, Medicare, and state scope-of-practice and supervision rules |
Missing time documentation, weak medical necessity, missing treatment plans, and missing signatures are not theoretical concerns. They are the documented failure patterns in real Medicare audits. (CGS Medicare)
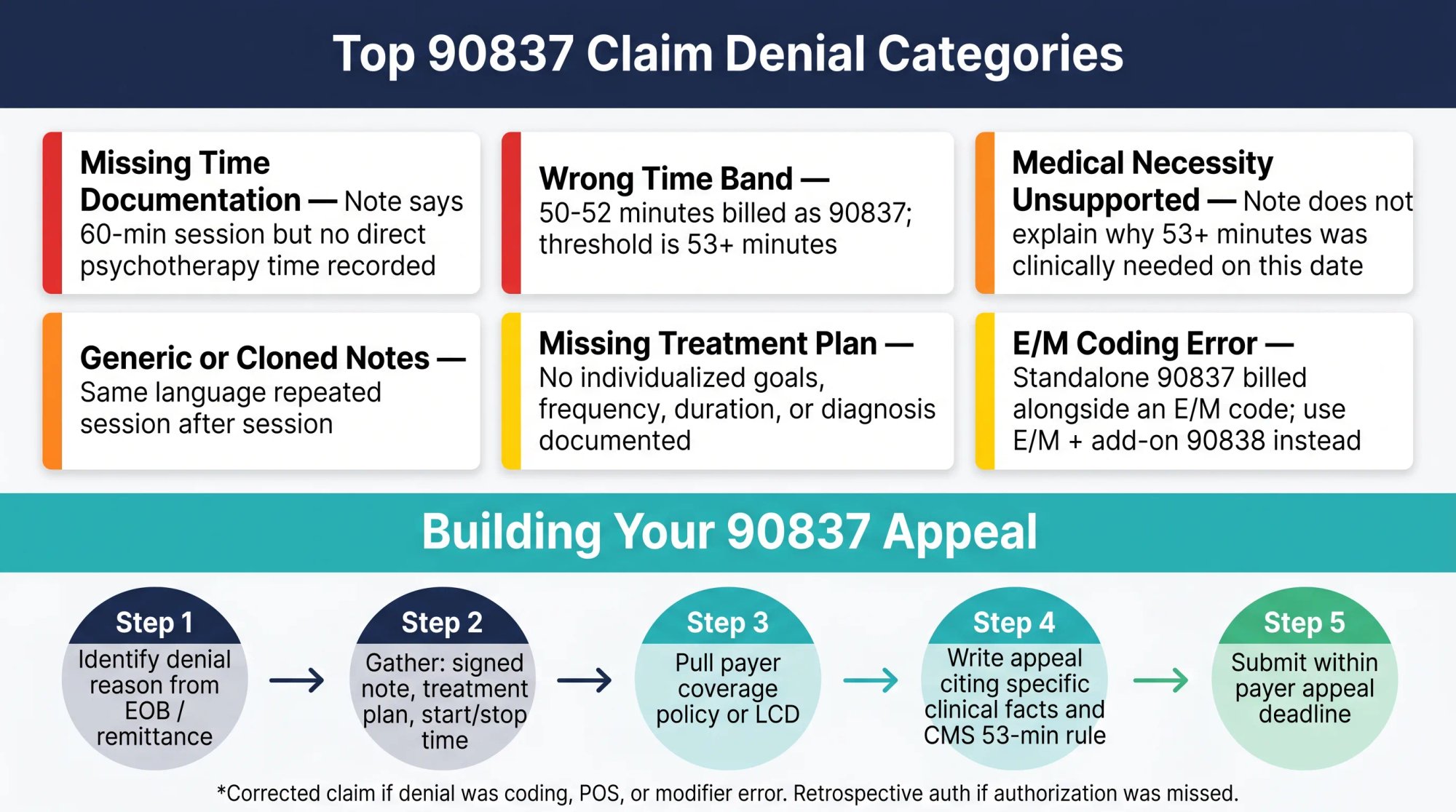
What to include in a 90837 appeal packet
When a 90837 claim is denied and the documentation supports the service, the appeal packet should include:
- The denied claim and explanation of benefits (EOB)
- The payer's stated denial reason
- The payer's relevant coverage policy or LCD, if available
- The signed progress note
- The active treatment plan
- Start/stop or total psychotherapy time documentation
- Diagnosis and medical-necessity support
- Telehealth documentation, if applicable
- The authorization number, if one was obtained
- Rendering-provider credentialing or licensure documentation, if the denial was provider-related
- A corrected claim, if the denial was due to a coding, POS, or modifier error
Sample appeal language for a time-and-necessity denial:
CPT 90837 was billed because the progress note documents 57 minutes of direct psychotherapy from 2:03 PM to 3:00 PM. The patient was present throughout the service. The record supports medical necessity due to chronic PTSD, increased panic symptoms, work impairment, and moderate relapse risk. Documented interventions included trauma-focused CBT, grounding practice, relapse-chain analysis, and relapse-prevention planning. CMS billing guidance assigns psychotherapy of 53 minutes or more to CPT 90837 and requires start/stop or total time documentation, both of which are present in the submitted record.
90837 edge cases: late arrivals, crises, and other tricky scenarios
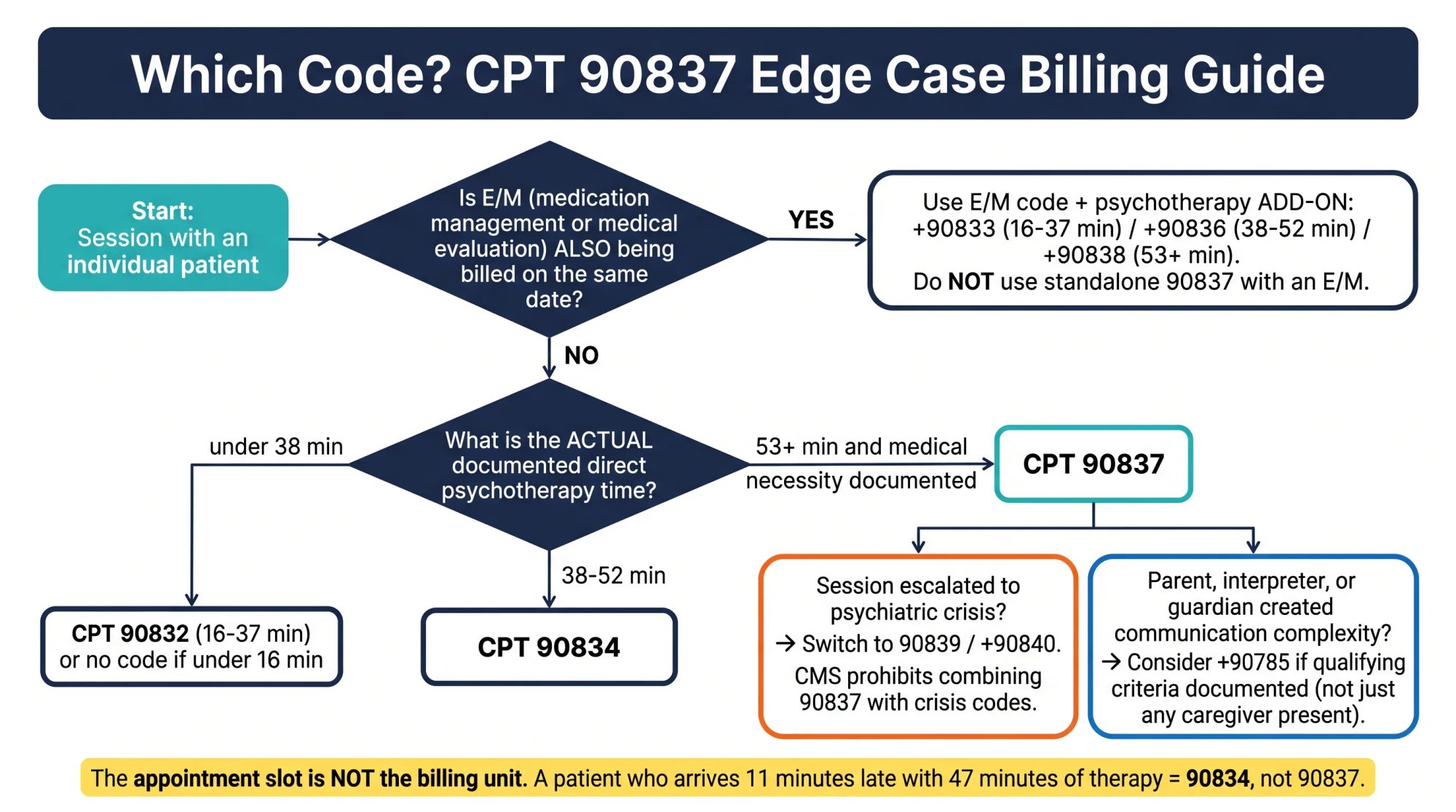
The patient arrives late
Scheduled 60 minutes. Patient arrives 11 minutes late. You provide 47 minutes of psychotherapy. Bill 90834, not 90837. The psychotherapy time was 47 minutes.
Session is exactly 53 minutes
Documented psychotherapy time is 53 minutes, and medical necessity supports an extended session. Bill 90837. You do not need 60 minutes.
Session is 52 minutes but clinically intense
Even if the session involved complex trauma work, suicidal ideation assessment, and detailed safety planning, if the documented psychotherapy time is 52 minutes, the correct code is 90834. Intensity does not override the time threshold.
Session runs 75 minutes for a non-crisis patient
Usually bill one unit of 90837. Do not assume you can bill multiple units of 90837 or add a prolonged-service code without verifying the payer's current policy. CMS's Medically Unlikely Edit program sets limits on units of a CPT code for the same provider, same patient, same date, and not all MUE values are publicly disclosed. (CMS MUE) If you regularly provide sessions exceeding 90 minutes: under Medicare billing guidance, a prolonged-service code may be reported alongside standalone 90837 when the psychotherapy service is 90 minutes or longer with direct patient contact, but prolonged-service codes should not be used with psychotherapy add-on codes billed alongside an E/M. For commercial plans, verify the payer's current policy before billing prolonged services.
The session becomes a psychiatric crisis
If a session escalates to a qualifying psychiatric crisis, acute safety risk requiring urgent assessment and stabilization, not simply a difficult or emotionally intense session, review whether crisis psychotherapy codes 90839 and +90840 apply. CMS guidance is explicit that crisis codes should not be reported alongside 90832 through 90838. (CMS) Use the right code family for the right type of service; do not try to stack them.
Psychiatrist provides medication management and 55 minutes of psychotherapy
Bill the appropriate E/M code (e.g., 99214) plus +90838 for the psychotherapy portion. The E/M time does not count toward the psychotherapy time. The standalone code 90837 is not used alongside an E/M code.
A parent joins an adolescent's individual therapy session
90837 can still be the correct code if the service remains individual psychotherapy and the patient is present for all or some of the session. Add +90785 only if qualifying interactive complexity criteria are present and documented, not simply because a caregiver participated.
Family-only session
If the patient is not present and the service is family psychotherapy without the patient, consider 90846, not 90837. (CMS)
Couples or family therapy with patient present
If the family or couple system is the treatment focus, not individual psychotherapy with family involvement, consider 90847. (CMS)
Group therapy
Use 90853. Not 90837.
Hospital, PHP, IOP, or SUD facility billing
In hospital outpatient departments, partial hospitalization programs (PHP), intensive outpatient programs (IOP), and SUD facility settings, 90837 billing involves additional layers. Professional claims may use CMS-1500/837P with CPT codes and provider NPIs, while institutional claims use UB-04/837I with revenue codes, facility billing rules, and payer-specific program requirements. Noridian lists revenue code 0914 for individual therapy in behavioral health institutional billing. (Noridian Medicare) Do not assume that office-based 90837 rules transfer cleanly to facility billing contexts.
What to check before submitting a 90837 claim
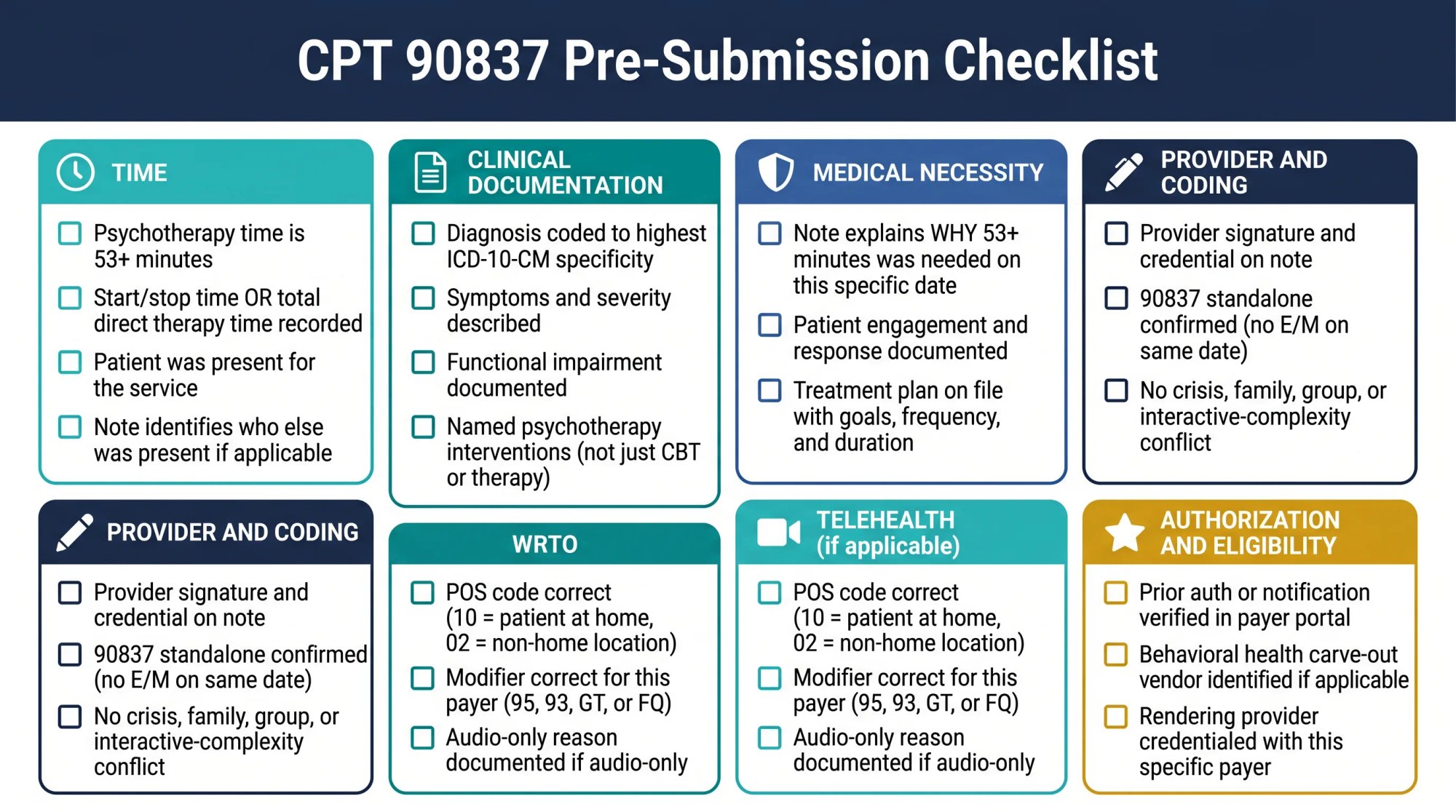
Before submitting a claim for 90837, confirm all of the following:
- Actual psychotherapy time was 53 minutes or more
- Start/stop time or total psychotherapy time is documented
- Patient was present for all or some of the service
- The note identifies anyone else who was present during the session
- Diagnosis is specific, coded to the highest ICD-10-CM specificity the record supports
- Symptoms and severity are documented
- Functional impairment is described
- Specific psychotherapy interventions are documented (not just "CBT" or "therapy")
- Patient response or engagement is noted
- The note explains why 53+ minutes was medically necessary for this patient, on this date
- An active treatment plan supports frequency, duration, goals, and diagnosis
- Provider signature and credential are present on the note
- POS code is correct for the setting and modality
- Telehealth modifier and modality are correct, if applicable
- Audio-only rules and documentation are addressed, if applicable
- Authorization or notification requirements for this plan were checked before the session
- Rendering provider is credentialed with the payer and eligible to bill this service
- No inappropriate E/M, crisis, family, group, or interactive-complexity code conflict exists
Why accurate 90837 billing matters beyond compliance
There is a broader point behind all of this technical detail.
CPT 90837 is a legitimate, medically appropriate code for one of the most clinically valuable service types in behavioral health: a full-length individual psychotherapy session. The goal of documentation is not to game a system. It is to accurately represent the care that was provided and to protect the provider, and the patient, if that care is ever reviewed.
The two things that must be true for every 90837 you bill: the session included 53 or more minutes of direct psychotherapy, and the patient's clinical situation on that date justified that extended time. Document both. Treat payer-specific rules on authorization, telehealth modifiers, add-on codes, and reimbursement as things to verify, not assume.
If you're billing 90837 regularly for a behavioral health or mental health practice, the documentation discipline described here is not theoretical. It is what payers actually check when they send the ADR. At Clarity Health RCM, behavioral health and mental health practices are among the specialties we serve, and 90837 is one of the codes we help practices document and defend correctly. If you want a billing team that understands psychotherapy coding at this level, we are glad to talk.
Frequently asked questions about billing 90837
Is CPT 90837 always a 60-minute session?
No. CPT 90837 is commonly called the "60-minute psychotherapy code," but the actual CMS billing threshold is 53 minutes or more. A 53-minute session with documented time and clinical justification qualifies for 90837. A session scheduled for 60 minutes but containing only 50 minutes of direct psychotherapy is 90834. (CMS)
Can I bill 90837 every week for the same patient?
Yes, if each session genuinely includes 53 or more minutes of psychotherapy and the clinical record supports the extended duration. Billing 90837 every week for every patient without individualized documentation is the pattern payers flag. Weekly 90837 is defensible when the treatment plan and session notes consistently show why the patient's diagnosis, severity, and functional impairment require 60-minute-level sessions rather than 45-minute sessions. (CarePaths)
What happens if my session was 52 minutes?
Bill 90834. The 90837 threshold is 53 minutes. One minute below that threshold and the correct code is 90834, even if the session was clinically complex. There is no mechanism in CPT psychotherapy coding to round up to the next time band.
Does telehealth always use modifier 95 for 90837?
No. Modifier 95 is common for commercial telehealth claims using synchronous audio-video, but it is not universal. Medicare behavioral health telehealth may use modifier 95, or modifier 93 for audio-only services, or modifier FQ in certain contexts. Some Medicaid programs and legacy commercial plans still require modifier GT. Modifier rules vary by payer, product, and state. Verify the correct modifier in the payer's current telehealth billing policy before submitting.
Can a clinical social worker bill 90837?
Yes, if licensed and credentialed with the payer. Medicare identifies eligible billing providers for psychotherapy services as including clinical social workers, and most commercial payers credential licensed clinical social workers to bill psychotherapy codes including 90837. However, payment rules differ: Medicare pays clinical social workers at a different rate than physicians or clinical psychologists for certain services. Some Medicaid programs may have different modifier or supervision requirements for social worker billing. (CMS)
What is the difference between 90837 and 90838?
CPT 90837 is the standalone individual psychotherapy code for 53+ minutes, used when psychotherapy is the only service on that date. CPT +90838 is the add-on psychotherapy code for 53+ minutes, used when psychotherapy is provided with a separately identifiable E/M service (medication management, medical evaluation) on the same date. You cannot bill 90837 alongside an E/M code. (CMS)
Can I bill 90837 and 90785 together?
Yes, when interactive complexity criteria are met. CMS allows +90785 to be reported with 90837 when the session involves qualifying communication factors such as involvement of legal guardians, interpreters, child welfare agencies, or caregiver emotions interfering with treatment. Interactive complexity is not a "difficult session" add-on. It requires documentation of the specific qualifying factor and time. (CMS)
What is the MUE for 90837?
CMS's Medically Unlikely Edit program sets maximum expected units of a CPT code for the same provider, same patient, and same date. Not all MUE values are publicly disclosed. In general, 90837 is billed as one unit per date of service. Attempting to bill two units of 90837 for a longer session without explicit payer guidance and supporting policy is likely to trigger a MUE denial or medical review. (CMS MUE)
Does Medicare require prior authorization for 90837?
Traditional Medicare fee-for-service generally does not require prior authorization for routine outpatient psychotherapy including 90837. However, Medicare Advantage plans may have different prior authorization requirements. And all Medicare fee-for-service psychotherapy claims remain subject to medical necessity documentation rules, post-payment review, Medicare Administrative Contractor (MAC) audits, and MUE edits, so "no prior auth" does not mean no documentation scrutiny.
What should I do if a 90837 claim is denied?
First, identify the specific denial reason from the EOB or remittance advice. Then gather the supporting documentation: the progress note with time and medical necessity, the active treatment plan, and the relevant payer policy. If the documentation supports the service and the denial is for medical necessity or time documentation, build your appeal around the specific clinical facts from that session and the CMS time-band guidance for 90837. If the denial is for a coding, modifier, or POS error, submit a corrected claim. If it is an authorization issue, check whether a retrospective authorization is possible and what the payer's deadline for appeal submission is.
No responses yet