Charge capture sounds administrative. In hospital finance, it's anything but. One healthcare audit source estimates that organizations lose 3% to 5% of net revenue annually from charge-capture errors, and for a hospital with $500 million in annual net revenue, that puts roughly $15 million to $25 million at risk each year, according to Heidi Health's charge capture overview.
That number changes the conversation. What is charge capture? It's not a billing footnote. It's an operating control that determines whether the care your teams deliver makes it onto a defensible, payable claim. When leadership treats it as a narrow billing task, revenue leaks through documentation gaps, coding mismatches, charge lag, and broken handoffs between clinical and revenue cycle teams.
Table of Contents
- The Multi-Million Dollar Question What Is Charge Capture
- Beyond Billing The Core Concept of Charge Capture
- The Journey of a Charge From Clinic to Claim
- Common Leaks Why Good Charge Capture Processes Fail
- Key Metrics to Measure Charge Capture Health
- Building a Leak-Proof Charge Capture Process
- Your Path to Financial Clarity and Revenue Integrity
The Multi-Million Dollar Question What Is Charge Capture
If a hospital delivers care but fails to turn that care into an accurate claim, finance doesn't see a documentation issue. Finance sees margin erosion.
That's why the right answer to what is charge capture starts with business risk, not terminology. Charge capture is the process of identifying, documenting, coding, and submitting every billable service, procedure, supply, and medication tied to a patient encounter so the organization can bill correctly and avoid missed revenue. In practical terms, it sits at the front end of revenue integrity. It's where clinical activity becomes financial data.
Leadership teams often underestimate the cumulative effect of “small” misses. A supply not recorded in the EHR. A procedure note signed late. A medication administration that never reaches the claim. A diagnosis that supports treatment clinically but wasn't documented with enough specificity to support billing. None of these looks dramatic on its own. In aggregate, they become a recurring loss pattern.
Charge capture should be managed like a control environment, not a clerical workflow.
The compliance side matters just as much. Charge capture has to align clinical documentation with CPT and ICD coding, along with dates, locations, and supplies used, so the claim can withstand payer review and audit scrutiny. When that alignment breaks, the organization doesn't just miss reimbursement. It also creates avoidable denial work, rebilling effort, and audit exposure.
For executives, the issue is straightforward. If your teams can't consistently answer whether all billable care was captured completely, accurately, and on time, then you have a revenue integrity problem whether denials have surfaced yet or not.
Beyond Billing The Core Concept of Charge Capture
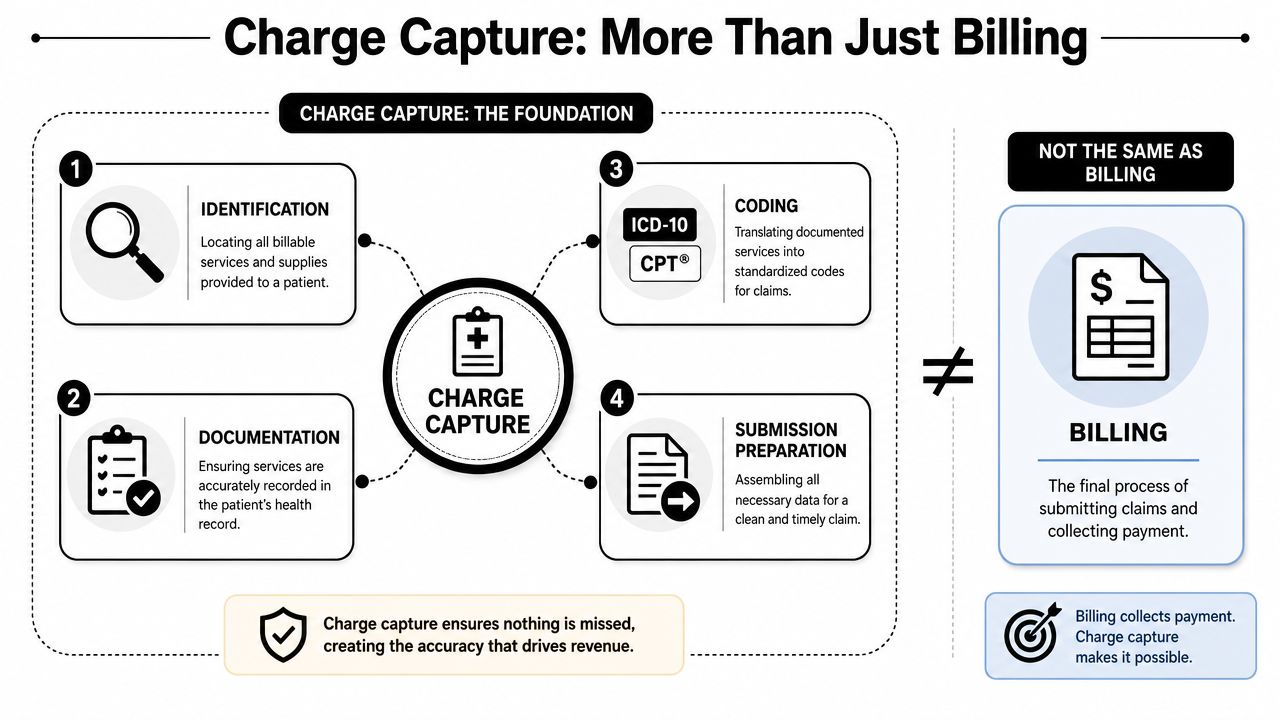
When “charge capture” is mentioned, “billing” often comes to mind. That's the first misconception to remove.
Charge capture is not just coding or billing. It is the point-of-care process of identifying every billable service, supply, and medication so those items can later be coded and reimbursed, and gaps here create both missed revenue and compliance risk, as described by Definitive Healthcare's glossary entry on charge capture.
What gets captured
A useful way to think about charge capture is as the itemized record behind a complex clinical encounter. Not a retail receipt, but the operational equivalent. It should reflect what was done, what was used, and what supports medical necessity.
That usually includes:
- Professional services: Evaluation, procedural work, interpretation, and other clinician effort that must be documented clearly enough to support coding.
- Supplies and devices: Kits, implants, disposable items, and other billable materials that can disappear from reimbursement if they aren't tied back to the encounter.
- Medications: Drugs administered during care, especially in settings where high-volume medication activity creates many opportunities for variance.
- Visit context: Diagnosis details, place of service, timing, units, and other encounter metadata that determine how the claim is built.
Why this is different from billing
Billing comes later. Billing submits the claim and pursues payment. Charge capture creates the raw material the claim depends on.
That distinction matters because many organizations focus their improvement effort too far downstream. They invest heavily in claim edits and denial follow-up while leaving the point-of-care capture process inconsistent. That approach can recover some defects, but it won't rescue services that were never documented or entered in the first place.
A sound charge capture process answers a simple question with discipline: did the record reflect the full scope of care delivered? If the answer is uncertain, coders guess, billers chase clarifications, and finance receives a distorted view of earned revenue.
Practical rule: If a service, supply, or medication can't be traced cleanly from the medical record into the claim workflow, assume there's leakage until proven otherwise.
The Journey of a Charge From Clinic to Claim
A charge doesn't appear on a clean claim by accident. It moves through a chain of documentation, coding, validation, and payer-facing steps. Every handoff is a control point.
Charge capture is the operational control layer that converts documented clinical activity into billable claims. In practice, it must reconcile services, supplies, medications, diagnosis codes, and visit metadata before claim submission, and the process spans documentation, coding, and billing, as outlined in Nextech's explanation of charge capture.
Start with the workflow map:
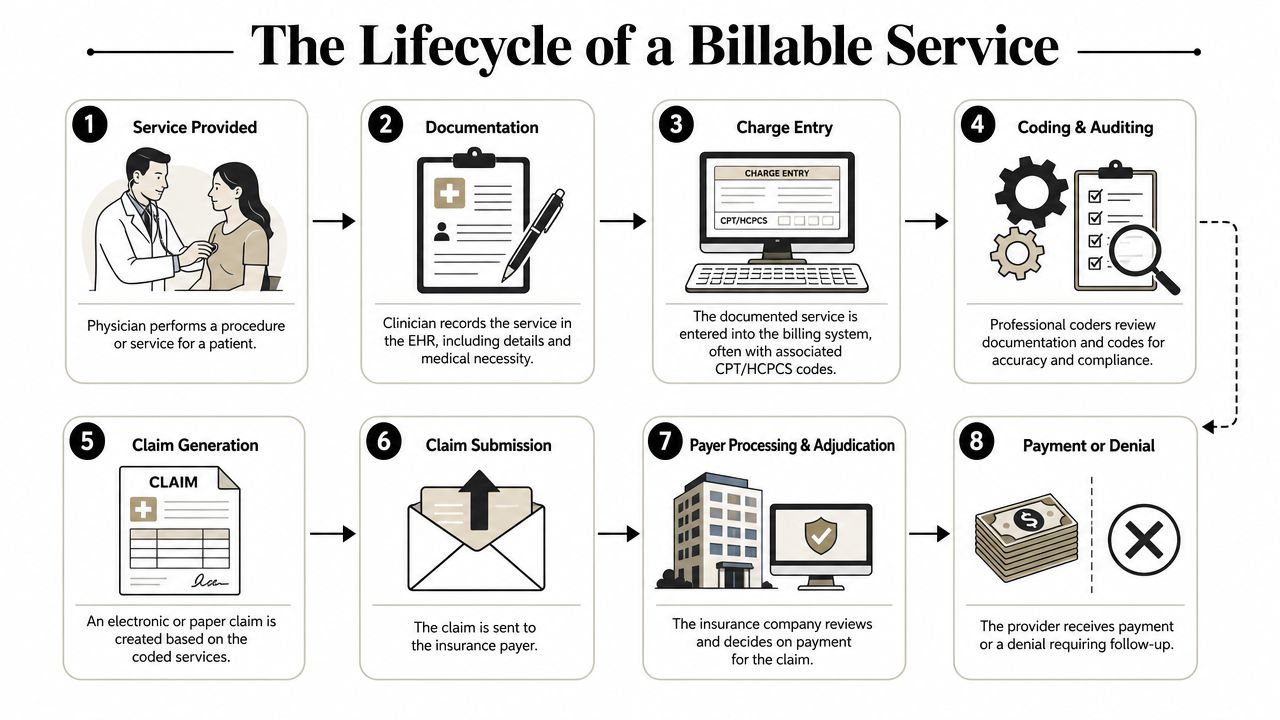
A single encounter through the workflow
A patient arrives for treatment. The clinician performs an evaluation, orders or performs a procedure, uses supplies, administers medication, and documents the encounter in the EHR. At that moment, charge capture begins. The record has to reflect enough detail for downstream staff and systems to identify what is billable.
From there, the encounter typically moves through a sequence like this:
- Clinical documentation happens at or near the point of care. If the note is late, vague, or incomplete, every later step gets harder.
- Charges are linked or entered. Some organizations rely on charge tickets or manual entry. Others use EHR triggers, charge routers, or structured templates.
- Coding staff review the documentation. They map the encounter to the correct CPT, HCPCS, and ICD logic supported by the record.
- The charges are reconciled against billing rules. At this stage, units, modifiers, supply detail, and chargemaster alignment matter.
- The claim is generated and submitted. After that, the payer adjudicates it. If you want a plain-language overview of that payer decision step, see this explanation of claim adjudication.
Here's a short explainer for teams that need a visual walkthrough before redesigning the workflow:
Where handoffs break
The weakness usually isn't one catastrophic failure. It's cumulative friction between teams and systems.
| Handoff | What commonly goes wrong | Likely downstream result |
|---|---|---|
| Clinician to EHR | Incomplete note, missing supply detail, late signature | Under-coding, missing charges, billing delay |
| EHR to coding | Ambiguous documentation or unsupported service detail | Clarification requests, rework, claim edits |
| Coding to billing | Units, modifiers, or visit metadata not aligned | Claim rejection, underpayment, denial |
| Billing to payer | Incomplete or inconsistent claim lines | Delayed adjudication or denial |
Hospitals that handle this well don't rely on heroics from coders or billers. They design the workflow so the charge is captured close to care delivery, validated quickly, and reconciled before defects spread downstream.
Common Leaks Why Good Charge Capture Processes Fail
Charge capture failures rarely announce themselves as “we are losing revenue here.” They show up as late charges, recurring manual corrections, unexplained variance by department, or a denial pattern that looks like a coding issue when the root cause sits earlier in the workflow.
A peer-reviewed review of charge capture methods describes controls such as comparing drug purchases versus charges, comparing dispensing records versus billing records, and reconciling encounter forms against billed items. The same source also notes that ineffective charge capture can lead to up to 1% of net charges being lost, while one organization achieved a $7.8 million revenue increase after improving charge-capture analytics, according to the PMC review of charge capture methods.
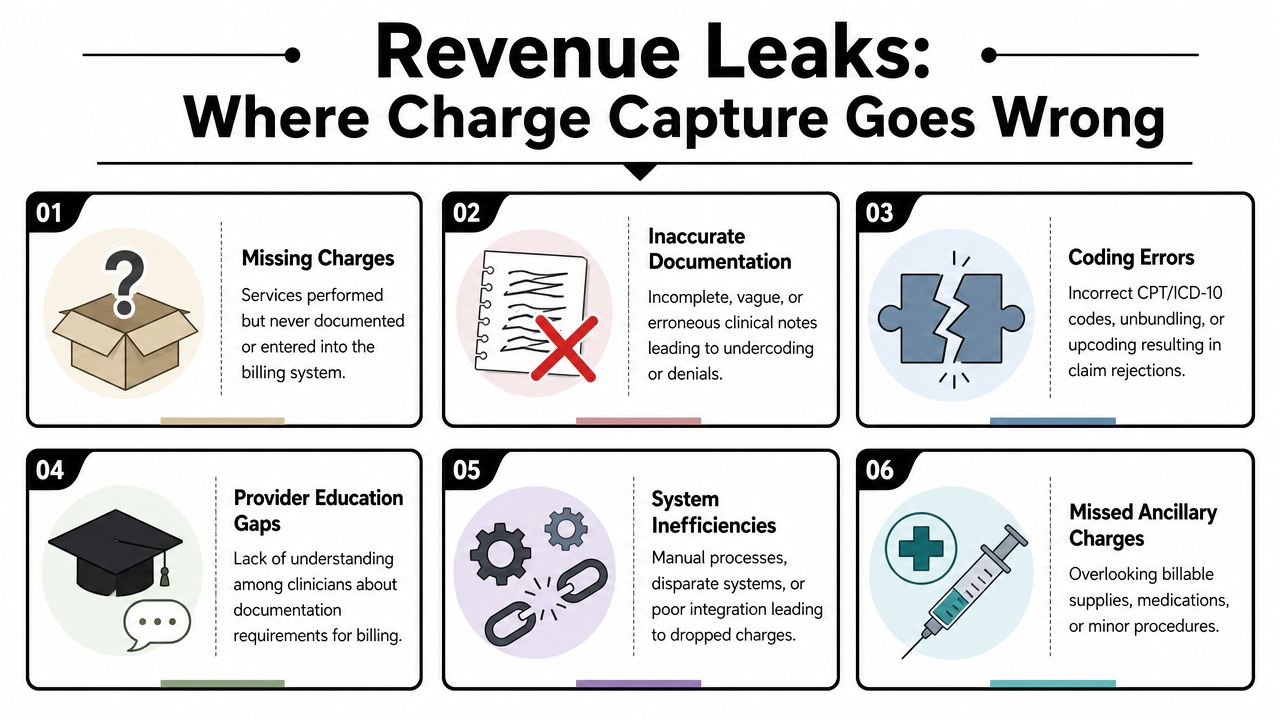
The failures that quietly drain margin
Some leaks are obvious. Many are operationally mundane.
- Missing ancillary charges: Supplies, medications, or minor procedures often fall outside the provider's main note and depend on nursing, procedural, or dispensing documentation. If those records don't reconcile to the claim, the organization doesn't bill for work already performed.
- Documentation that supports care but not billing: Clinical teams may document treatment appropriately for patient care yet omit the detail needed to support coding specificity, units, or medical necessity. That creates either under-coding or payer challenge.
- Charge lag: When charges are entered well after the encounter, staff rely on memory, paper notes, or late chart completion. Accuracy drops, and the risk of filing delays rises.
- Workflow fragmentation: Different departments may use different capture methods, edit queues, or ownership rules. That inconsistency makes enterprise oversight weak and root-cause analysis slow.
- Overdependence on downstream cleanup: If coders and billers spend their time correcting front-end defects, the organization has built a rework machine instead of a reliable capture process.
What bad process looks like in practice
Consider a medication-heavy department. Pharmacy has dispensing records. Nursing has administration documentation. Billing has claim lines. If those three data sets aren't reconciled regularly, variance can hide across a large transaction volume for a long time.
Or take surgery and procedural areas. The main procedure may be captured cleanly, while implants, time-based elements, assistant participation, or related supplies are documented in separate places. The claim goes out looking complete because the core procedure is there. Finance doesn't notice the leakage until someone compares clinical activity to billed detail.
The most expensive charge capture failures are usually the ones that still produce a payable claim. They don't trigger urgent denial work, so they sit in the background as accepted underbilling.
When these patterns appear, leadership shouldn't ask only whether claims are going out. It should ask whether the billed record fully matches the care record. Organizations that need to quantify and recover leakage often pair charge-capture diagnostics with broader medical revenue recovery work so they can isolate what was missed, what can still be corrected, and which departments need tighter controls.
A practical diagnostic checklist looks like this:
- Trace selected encounters end to end: Follow the visit from clinical record to detailed bill and compare what was done against what was charged.
- Reconcile high-risk categories: Focus first on drugs, supplies, procedural departments, and high-variation services.
- Review late-charge patterns: Repeated late posting usually points to a broken handoff, not a one-off staff mistake.
- Separate under-coding from non-capture: They look similar in financial reports but require different fixes.
Key Metrics to Measure Charge Capture Health
If finance wants control, it needs a charge capture dashboard that shows completeness, timeliness, and downstream impact. The mistake many hospitals make is tracking denials only after claims fail. By then, the process has already broken.
Industry guidance frames charge capture as a measurable process that should be monitored with KPIs such as missed charges identified and recovered, charge lag time, and revenue per encounter. That's the right starting point for executive oversight.
Use this dashboard as the visual baseline:
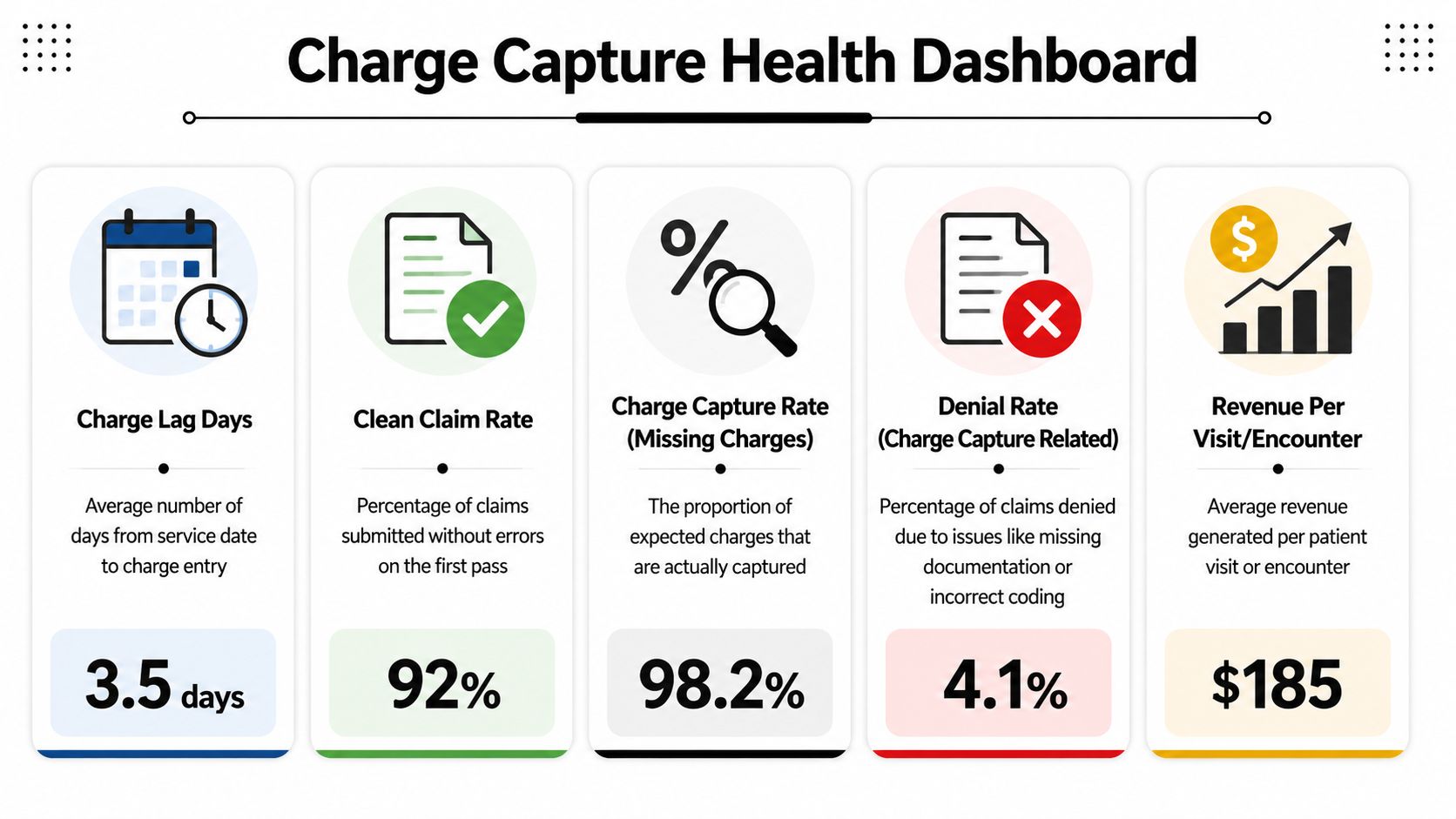
The dashboard leadership should review
Rather than chase one master metric, review a small set that exposes different failure modes.
| Metric | What it tells you | Warning sign |
|---|---|---|
| Charge lag time | How quickly encounters become billable charges | Growing lag by department or provider |
| Missed charges identified and recovered | Whether audits are finding real leakage | Recoveries stay high month after month |
| Revenue per encounter | Whether capture patterns are stable across service lines | Unexplained drop without volume or payer shift |
| Denials tied to documentation or coding support | Whether capture defects are surfacing at adjudication | Repeated preventable denial reasons |
| Late charges | How often revenue is posted after the expected window | Chronic late activity in the same units |
What the trends usually mean
A single bad week doesn't prove a broken system. Persistent patterns do.
If charge lag increases while denial work also rises, the problem is often upstream documentation discipline or weak ownership at handoff points. If revenue per encounter drifts downward in one specialty while utilization appears stable, review under-capture before assuming payer mix caused it. If the same missed-charge categories keep being “recovered” in audits, then the audit is acting as a patch, not a control.
Healthy charge capture operations don't just find errors. They reduce the need to keep finding the same errors.
For CFOs, the most useful reporting cadence is one that compares departments against their own baseline and flags variance quickly enough for operational correction. Raw billing volume won't tell you that. Encounter-level analytics will. Teams looking to operationalize this usually combine charge lag, reconciliation results, and denial reasons in a shared healthcare revenue cycle analytics view so finance, revenue integrity, and department leaders are looking at the same facts.
Building a Leak-Proof Charge Capture Process
Hospitals don't fix charge capture with a memo, a one-time training session, or a new edit queue. They fix it by redesigning the operating model around standardization, fast validation, and clear ownership.
Neutral sources note that charge capture issues can affect up to 1% of net patient revenue in hospitals, and recent guidance stresses automated review and standardization as the response to prevent leakage at scale, according to Combine Health's discussion of charge capture in healthcare RCM.
Technology helps but workflow discipline matters more
EHR-integrated automation is useful when it reduces reliance on memory and manual handoff. Charge linking, flowsheet logic, and procedure-note triggers can help surface expected billable activity. Reconciliation tools can compare what clinical systems recorded against what billing systems received. Real-time discrepancy flagging can shorten the correction cycle.
But technology alone won't solve bad governance. If a department hasn't defined who owns supply documentation, who reviews charge exceptions, or how quickly charge lag must be resolved, the software will mostly generate better visibility into an old problem.
The operating model that works
The strongest charge capture environments usually share the same design principles:
- Standardize at the point of care: Use structured templates, charge prompts, and specialty-specific workflows that reflect how the department delivers care.
- Audit where leakage is most likely: Medication-heavy units, procedural areas, and service lines with many ancillary charges deserve tighter reconciliation routines.
- Create short feedback loops: When coding or billing teams find recurring documentation defects, the information has to get back to the clinicians and managers who can change the process.
- Separate prevention from cleanup: Denial management matters, but it shouldn't substitute for front-end control.
- Assign accountable owners: Someone has to own charge lag, someone has to own reconciliation, and department leadership has to own repeated exceptions.
One practical option is to pair internal revenue integrity leadership with an outside operating partner that can handle workflow analysis, billing operations support, and targeted gap closure. For organizations that want that structure, Clarity offers full-service and a la carte revenue cycle support across the billing workflow, including charge capture-related operational functions.
Your Path to Financial Clarity and Revenue Integrity
Charge capture isn't a narrow billing definition. It's the control system that determines whether documented care becomes earned revenue with compliance support behind it.
When hospital leadership asks what is charge capture, the useful answer is this: it's the point where clinical reality is either translated accurately into billable data or lost through process failure. That makes it a finance issue, an operations issue, and a compliance issue at the same time.
The organizations that improve it don't start with abstract transformation language. They start by tracing the workflow, isolating failure points, measuring charge lag and missing-charge patterns, and standardizing how departments document and reconcile billable activity. They also stop assuming that downstream claim edits can repair front-end omissions. They can't.
For CEOs, CFOs, and physician leaders, the next move is practical. Determine where charge capture ownership sits today. Review whether departments follow a common workflow or a patchwork of local habits. Look at where clinical documentation, coding review, and billing preparation disconnect. Then decide whether your team has the time and internal capacity to redesign it thoroughly.
A disciplined charge capture process protects revenue already earned. It also gives leadership a more accurate view of service-line performance, operational discipline, and financial integrity.
If you want an outside review of where charges are leaking, Clarity can provide a complimentary consultation of your current revenue cycle and help map a customized plan to improve charge capture accuracy, workflow efficiency, and overall profitability.
2 Responses
[…] drag usually starts upstream. Weak documentation, inconsistent charge entry, and gaps in charge capture workflows often feed the coding queue with incomplete or conflicting information. Coding then works like a […]
[…] your teams still treat charge capture as a coding issue only, review how charge capture affects revenue integrity. The problem usually starts upstream in workflow […]