Your leadership team already feels the symptoms. Medicare Advantage volume is steady, patient complexity looks high, physicians are busy, yet revenue doesn't line up with the acuity you know you're managing. Finance sees unexplained variation. Clinical leaders insist the care is there. Coders are chasing notes after the fact. That gap is usually not a patient mix problem. It's an HCC program problem.
Most organizations treat hierarchical condition categories as a coding project. That's too small. HCCs sit at the intersection of documentation, physician workflow, compliance, and executive finance. If you manage them like a back-office task, you'll get back-office results. If you manage them like a strategic asset, you can stabilize reimbursement, strengthen audit defensibility, and make your revenue reflect the actual burden of care.
Table of Contents
- What Are Hierarchical Condition Categories
- The Financial Impact of HCCs on Your Practice
- Mastering Documentation and Coding Best Practices
- Building a Compliant Program and Avoiding Audits
- Optimizing Workflows and Technology for HCC Capture
- Measuring Your HCC Program's ROI and Key KPIs
What Are Hierarchical Condition Categories
Hierarchical condition categories are the payment logic behind risk-adjusted reimbursement. CMS established HCCs in 2004 as a core part of its risk adjustment payment model, and that model has been used annually to identify people with serious acute or chronic conditions and project expected care costs, as outlined in this CMS-HCC overview from IMO Health.
For leadership, the simplest analogy is car insurance. A driver with more risk factors costs more to insure. A patient with more documented clinical complexity costs more to manage. Medicare Advantage and related risk-adjusted models use HCCs to translate that complexity into payment. If your documentation understates the patient's condition burden, payment understates it too.
Why hospital leaders should care
The HCC system isn't built from every diagnosis code in the book. It maps approximately 9,500 of the 70,000 ICD-10-CM codes into 79 distinct categories, according to the American Society of Anesthesiologists' explanation of HCC coding. That means two things matter more than is often acknowledged:
- Clinical specificity matters: vague diagnoses often fail to reflect the true burden of care.
- Documentation matters more than problem lists: if the note doesn't support the condition clearly, the code won't hold up.
- Annual recapture matters: chronic disease stability doesn't protect next year's risk score.
If your executives still think HCCs belong only to coding, they're missing the point. HCC performance shapes how accurately the organization gets paid for the patients it already treats.
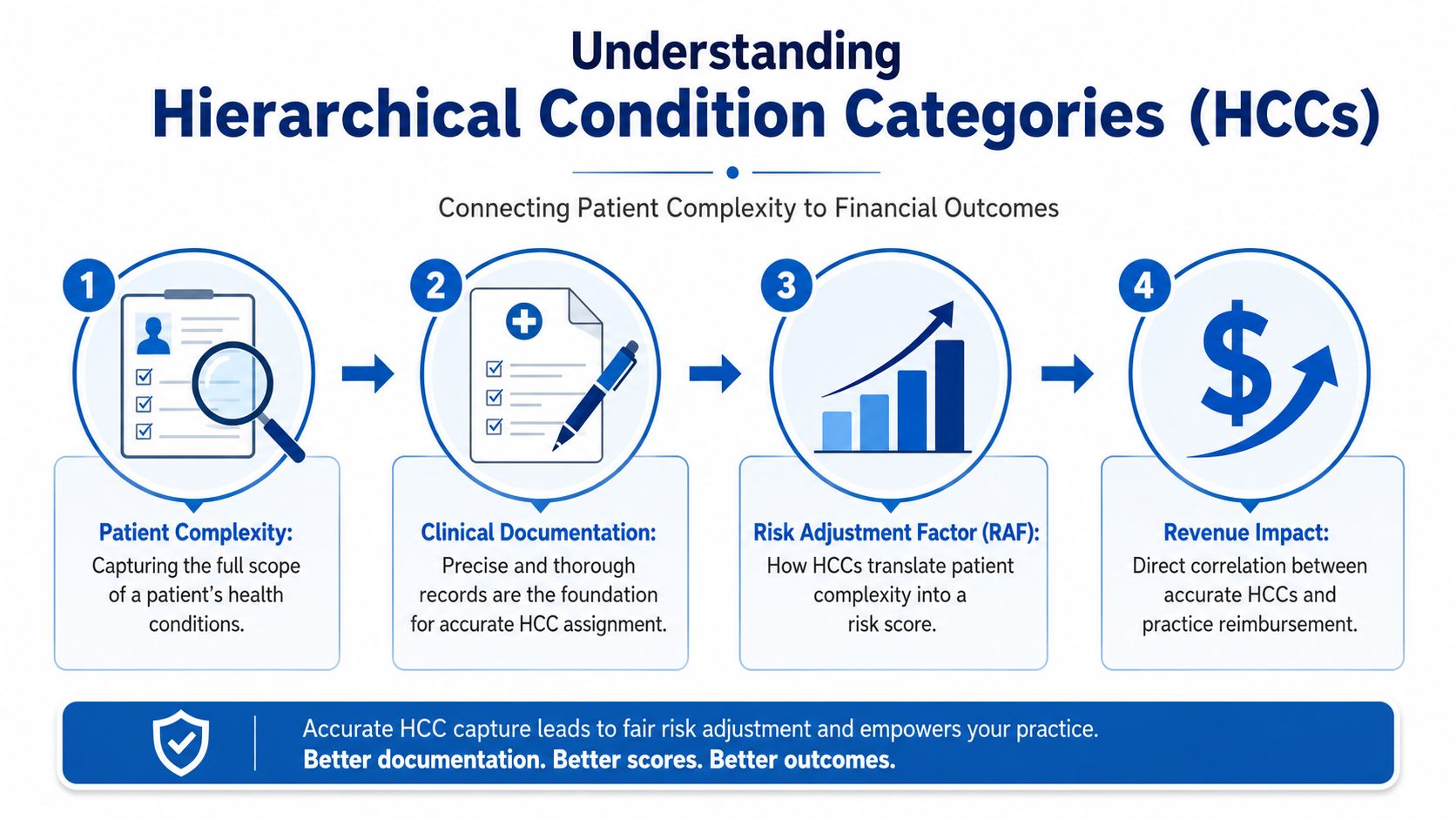
A patient's diagnoses feed into a Risk Adjustment Factor, or RAF, which is the score tied to expected cost and payment. If your physicians need a quick refresher on how that score works in practice, this RAF score overview is a useful companion.
How the hierarchy actually works
The word "hierarchical" is where many people get lost. The logic is simple. Within a related clinical family, only the most severe condition counts. CMS designed it that way to prevent double-counting of closely related diagnoses. If a patient has multiple related diagnoses in the same hierarchy, the highest-severity HCC is the one that drives the score.
Practical rule: HCC coding rewards accuracy, not diagnosis volume. More codes don't automatically mean more value.
That distinction matters operationally. A bloated note with loosely documented conditions isn't a strategy. A concise note with clinically supported severity is. The strongest HCC programs train physicians to document the active condition, current status, and management in a way that reflects the patient's real complexity without overstating anything.
There's one more point leadership can't ignore. Risk scores reset annually. If a chronic condition isn't documented again in a qualifying way during the year, it can fall out of the current risk profile even when the patient is still being treated for it. That's why HCC performance depends on disciplined workflows, not physician memory.
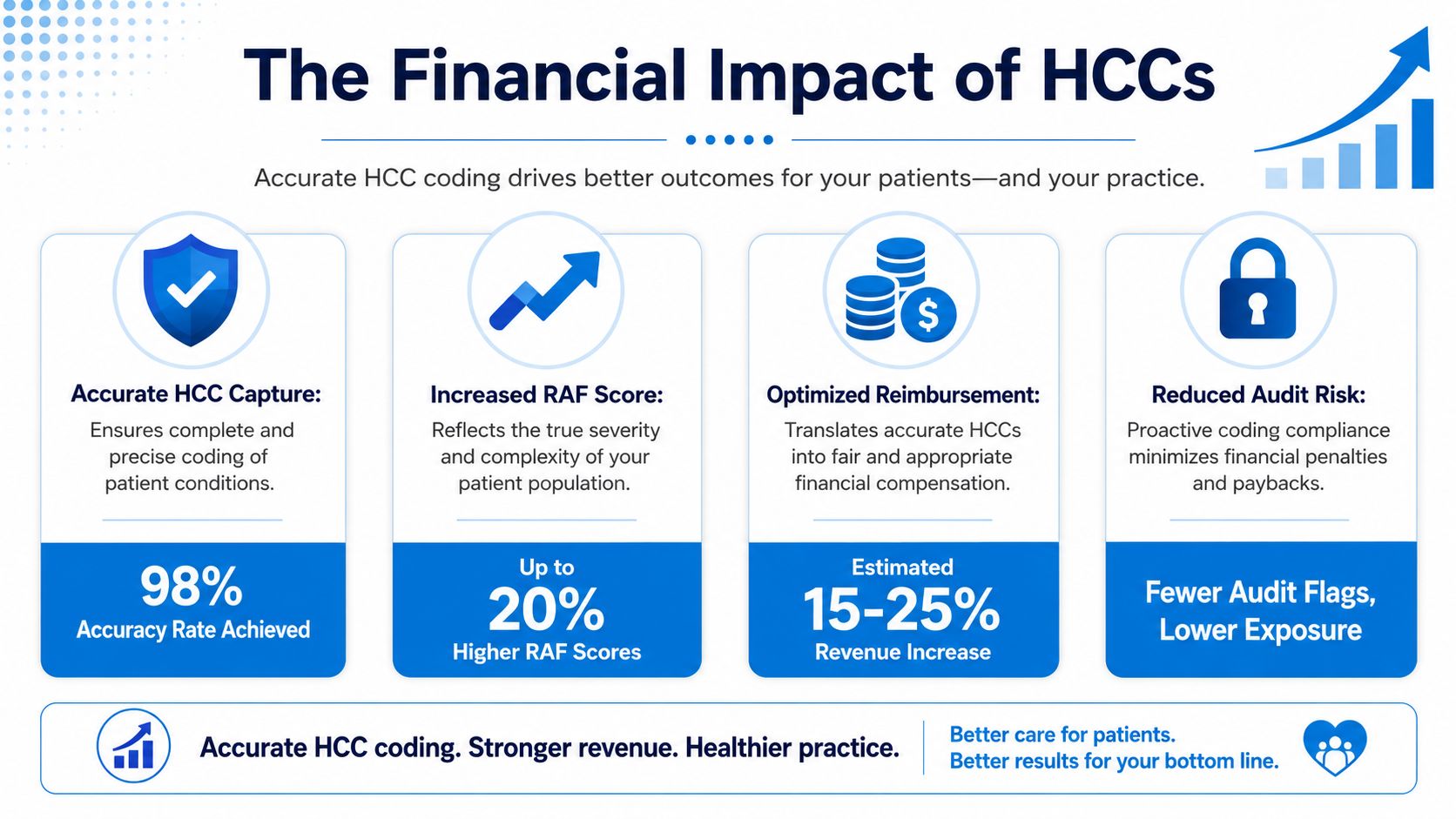
The Financial Impact of HCCs on Your Practice
Monday morning. Your CFO is reviewing next year's Medicare Advantage revenue forecast. Your physicians are seeing the same complex patients they saw last year, but projected reimbursement is lower, variance is wider, and no one can explain the gap with confidence. In many hospitals and medical groups, that gap starts with HCC performance.
HCCs affect far more than claim accuracy. They shape revenue forecasting, payer performance, physician compensation conversations, and the credibility of your financial plan. If documented risk is lower than true patient complexity, your organization gets paid for a healthier population than the one your clinicians are treating.
That is a finance problem.
Why leadership should treat HCCs as a strategic revenue function
An HCC program should sit at the intersection of clinical operations, coding, compliance, and finance. When those groups work in silos, revenue leaks out in predictable ways. The payer receives an incomplete picture of disease burden. Finance builds budgets on understated acuity. Physicians hear complaints about missing diagnoses but never see the enterprise impact.
Leadership needs a tighter model. Tie documentation quality to reimbursement integrity, then measure it like any other financial process.
| Executive concern | What weak HCC capture causes |
|---|---|
| Budgeting | Revenue projections become less reliable |
| Contract performance | Risk-adjusted payment may understate the acuity of your population |
| Physician alignment | Finance blames coding, physicians blame payer complexity |
| Compliance exposure | Teams may try to "fix" gaps late, with weaker documentation support |
Late-cycle cleanup is a warning sign, not a strategy. If your team is chasing unsupported diagnoses months after the visit, the failure happened at the point of care, not in the back office. Many of those breakdowns start with preventable medical coding errors that distort reimbursement and increase rework.
Where the money is gained or lost
The financial effect of HCCs rarely appears as one dramatic write-off. It shows up in small misses that stack up across a panel, a service line, or a full contract year. Under-documented chronic disease lowers risk-adjusted reimbursement. It also weakens your case in contract discussions because your reported population looks less complex than it is.
Here is the executive view. Two organizations can have similar physicians, similar patients, and similar visit volume. One organization documents active chronic conditions with clear assessment and plan language during the encounter. The other depends on copied problem lists, vague diagnoses, and year-end review projects. The first protects revenue with defensible documentation. The second leaves money on the table, then raises audit risk by trying to recover it after the fact.
This is why leadership should stop treating HCCs as a coding education project. It is a margin protection program with compliance constraints.
This short video helps frame that payment connection for teams that need a quick operational overview.
Fair payment is about making reimbursement match the complexity your clinicians manage.
Ask a better executive question. Stop asking, "How many codes are we missing?" Ask, "How much clinically supported complexity are we failing to convert into accurate reimbursement, and what is that costing us by contract, provider, and payer?" That question gets physicians, compliance leaders, and finance teams working toward the same outcome.
Mastering Documentation and Coding Best Practices
Most HCC programs fail in the note, not in the billing system. Physicians often know the patient is complex. Coders often know which conditions may matter. But if the encounter note doesn't show active management, the diagnosis becomes vulnerable. That's where organizations lose both revenue integrity and audit defensibility.
The fix isn't more generic education. It's a tight documentation standard built into daily workflow.
MEAT is the operating standard
For HCC-supported diagnoses, the note should show MEAT. That means the condition is being Monitored, Evaluated, Assessed, or Treated. If the documentation doesn't reflect that, a diagnosis can be challenged even if the patient has the condition.
That annual pressure is real. With risk scores resetting each year, providers face underpayment unless they implement real-time coding audits and documentation checklists that meet MEAT standards. Recent trends also showed that 30% of Medicare Advantage plans experienced RAF score declines due to documentation gaps, not patient health improvements, according to Clinii's HCC reference.
A lot of preventable leakage starts with basic note quality failures. These common medical coding errors often show up in HCC programs too, especially when providers use vague wording or rely on copied forward documentation.
What strong documentation looks like in practice
A compliant note doesn't need to be long. It needs to be specific and current.
- Diabetes example: Don't write "diabetes, stable." Document the current status, any complications being managed, medication or monitoring, and what you reviewed or adjusted during the visit.
- Hypertension example: Don't leave it as a problem-list mention. Note blood pressure assessment, medication review, response to treatment, and follow-up plan.
- Heart failure example: Don't settle for a generic reference if the condition is part of active management. Document the type when supported, current symptoms or absence of symptoms, treatment status, and your assessment.
A stronger note usually links three things. The diagnosis, the physician's clinical thought process, and the plan. That's what makes it useful for care, coding, and audit review.
If a diagnosis matters enough to influence payment, it should matter enough to appear clearly in the assessment and plan.
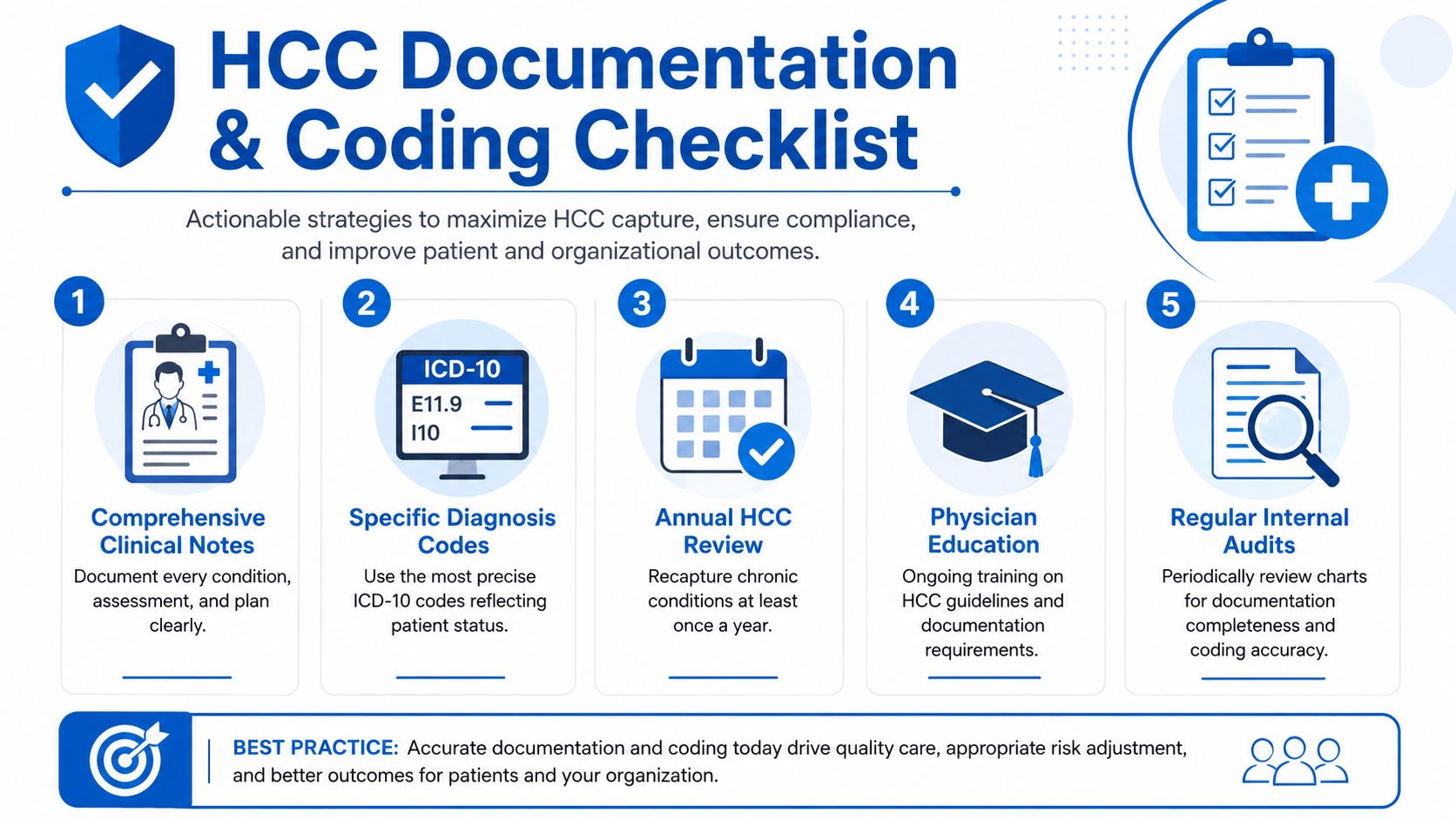
What to change tomorrow
Leadership doesn't need to wait for a major technology rollout. Start with operational discipline.
- Use pre-visit prep: Staff should identify prior chronic conditions that may need reassessment during the encounter.
- Standardize physician prompts: Build EHR templates that cue status, specificity, and management.
- Review in real time: Concurrent CDI or coding review is far more effective than retrospective rescue work.
- Close the loop with feedback: Show physicians where documentation failed and how to fix it in the next encounter.
- Separate stable from ignored: A condition can be clinically stable and still require active documentation if it's being monitored or treated.
Short checklist tools work better than long policy binders. Physicians respond to prompts embedded in Epic, Cerner, Meditech, or other EHR workflows. They rarely change behavior because someone emailed another PDF.
Building a Compliant Program and Avoiding Audits
A productive HCC program without compliance discipline is a future repayment project. Leadership should treat that as unacceptable. The same documentation gap that depresses reimbursement can also create audit exposure when unsupported diagnoses are submitted.
Compliance isn't the brake on HCC performance. It's the framework that keeps HCC performance real.

The red flags leadership should take seriously
Most audit vulnerability comes from familiar habits, not elaborate fraud schemes.
- Unsupported diagnosis capture: A code was submitted, but the note doesn't show active assessment or management.
- Cloned documentation: Prior language carries forward without proving that the condition was addressed at the current visit.
- Annual recapture failures: Chronic conditions disappear from valid current-year documentation and then reappear in rushed cleanup efforts.
- Unclear provider queries: Staff ask leading questions that look like revenue chasing instead of clarification.
- Overreliance on problem lists: The chart lists the condition, but the encounter doesn't support it.
These are governance problems. They usually reflect weak policy, inconsistent physician education, or pressure to repair risk capture late in the year.
What a defensible program includes
A solid compliance structure is operational, not ceremonial. It should include routine chart review, provider-specific feedback, escalation paths for repeat issues, and clear rules for when a diagnosis should be queried, coded, or left alone.
An effective governance model usually includes:
| Program element | What leadership should expect |
|---|---|
| Internal chart audits | Regular review of submitted diagnoses against encounter support |
| Provider education | Short, recurring training tied to actual documentation failures |
| Query policy | Clear standards for compliant clarification requests |
| Documentation standards | Defined expectations for assessment and plan language |
| Executive reporting | Visibility into trends by service line, clinic, and provider |
A compliant HCC program should be able to answer one question quickly: "Show me where this diagnosis was supported in the note."
If your team can't answer that quickly, the program is too dependent on hindsight. Leadership should push for prospective controls, not heroic retrospective recovery work.
Optimizing Workflows and Technology for HCC Capture
The fastest way to stall an HCC initiative is to tell physicians to "remember more." They won't. They shouldn't have to. Reliable HCC capture comes from workflow design that puts the right information in front of the right person before the note is signed.
That requires process first, then technology layered on top.
Build the workflow before you buy the software
Start with the patient journey. Before the visit, staff should review historical chronic conditions that may require reassessment. During the visit, the physician should see concise prompts for specificity and current management. After the visit, coding or CDI should review for support, not rewrite the clinical story.
A practical workflow looks like this:
- Pre-visit review: Flag prior HCC-relevant conditions for possible recapture.
- Point-of-care prompts: Use note templates, SmartPhrases, or condition-specific reminders inside the EHR.
- Concurrent review: Let CDI or coding staff identify missed opportunities while the encounter is still fresh.
- Exception handling: Route unsupported or ambiguous diagnoses back through a compliant clarification path.
- Leadership review: Monitor service lines that consistently miss annual recapture or generate unsupported codes.
Where technology actually helps
Technology earns its keep when it reduces dependence on memory and improves consistency. That can be as simple as structured templates in Epic or Cerner. It can also include natural language processing tools that scan the note and suggest conditions that appear clinically supported but not fully documented.
The larger strategic point is that better risk adjustment comes from broader context, not just diagnosis lists. A 7-year analysis of 653,815 patients found that an augmented CMS HCC model with demographic and socioeconomic characteristics had substantially greater predictive accuracy for outcomes such as length of stay and total charges than the standard model alone, as reported in this peer-reviewed analysis on PMC. Leadership should read that as a warning against simplistic HCC programs. The best organizations combine coding discipline with smarter patient stratification and operational planning.
If you're evaluating tools, compare them against your actual workflow problems. This healthcare RCM software guide is a useful starting point for thinking through where automation should support people instead of replacing judgment.
Technology should make it easier for physicians to document what they already know. It shouldn't push them into canned language that creates new audit risk.
Measuring Your HCC Program's ROI and Key KPIs
If leadership can't measure HCC performance, it will drift back into a coding side project. The scorecard should be operational enough for physician leaders and financial enough for the C-suite.
The KPI set leadership should review regularly
Track a small set of metrics consistently.
- Average RAF trend: Watch movement across the organization and by service line.
- Annual recapture rate: Measure how reliably prior chronic conditions are being documented again in the current year.
- Provider-level HCC capture patterns: Look for outliers, both low and high.
- Query response quality: Monitor whether clarification requests improve note support.
- Audit yield: Track how often internal reviews find unsupported diagnoses or missed supported conditions.
Don't let this become a vanity dashboard. If a KPI doesn't trigger action, remove it.
A simple ROI model executives can use
Use a straightforward model. Compare the cost of your HCC program against the financial impact of improved documentation integrity and reduced leakage. Include physician training time, CDI or coding support, EHR build work, and any software expense. Then compare those costs to changes in risk score performance, recapture consistency, and prevented compliance rework.
The point isn't to manufacture a flashy percentage. It's to prove whether the program is creating cleaner documentation, more accurate reimbursement, and lower downstream correction effort. That's the kind of ROI leadership should trust because it's tied to operational reality, not marketing math.
If your organization is treating hierarchical condition categories like a periodic cleanup task, you're leaving both money and control on the table. Clarity helps providers turn revenue cycle weak spots into disciplined, measurable performance, whether you need end-to-end support or targeted help with documentation, coding, and billing operations. A complimentary review of your current revenue cycle is the fastest way to see where HCC process failures are suppressing reimbursement and how to fix them.
No responses yet