About 80% of medical bills contain at least one error, and poor billing practices cost providers an estimated $125 billion annually according to Aptarro's medical billing statistics. That should change how you think about medical billing and practice management.
This isn't a back-office nuisance. It's the operating system for your cash flow.
If you're a new practice CEO, denials, slow payments, and unpredictable collections can feel like a billing problem. Usually, they start much earlier. The wrong insurance entered at scheduling. A missed authorization. Incomplete documentation. A payment posted without checking the payer contract. What looks like a collections issue is often a workflow failure upstream.
Table of Contents
- The Financial Engine of Your Healthcare Practice
- The Two Halves of Your Revenue Engine
- Your Revenue Cycle From Patient to Payment
- Why Revenue Leaks and Compliance Risks Emerge
- Measuring the Financial Health of Your Practice
- Deciding Between In-House and Outsourced RCM
- How to Choose the Right RCM Partner
The Financial Engine of Your Healthcare Practice
The practice management industry isn't small or sleepy. It's a projected $210.4 billion industry in 2026 in the United States, spanning 142,000 businesses, according to IBISWorld's medical group practice management industry data. CEOs who treat practice management as clerical overhead are managing a revenue engine like it's office furniture.
That mistake gets expensive fast.
A healthcare practice doesn't collect money because it delivered care. It collects money because it delivered care, documented it correctly, verified coverage, coded the encounter accurately, submitted a clean claim, followed up on payer behavior, posted payments properly, and billed the patient with discipline. Every one of those actions sits somewhere inside medical billing and practice management.
Why executives should care
Most new leaders focus on provider productivity, patient access, and hiring. Fair enough. But if your operational foundation is weak, growth magnifies defects instead of profit.
A fuller schedule won't save you if the front desk captures bad demographics. Adding physicians won't help if prior authorizations are missed. Strong clinical care won't protect margin if underpayments slip through posting unchecked.
Practical rule: Don't separate operations from revenue. In a medical practice, they're the same system viewed from different desks.
What smart operators do differently
They manage the practice like a business with one integrated financial engine.
That means:
- Scheduling is a revenue function. It determines whether eligibility, referrals, and authorizations happen on time.
- Clinical documentation is a revenue function. It determines whether coding stands up to payer scrutiny.
- Payment posting is an audit function. It confirms whether the practice was paid according to contract, not just whether cash hit the bank.
- Denial management is a feedback function. It tells you which upstream process is broken.
If you want a stable, profitable practice, stop thinking in departments. Think in handoffs. Revenue is won or lost at the transition points.
The Two Halves of Your Revenue Engine
The easiest way to understand medical billing and practice management is to stop treating them as separate disciplines.
Think of your practice like a restaurant. Practice management is the front of house. It handles reservations, seating, timing, guest flow, and service coordination. Medical billing is the back of house for finance. It turns the service into money, reconciles what should've been paid, and fixes exceptions when the system breaks.
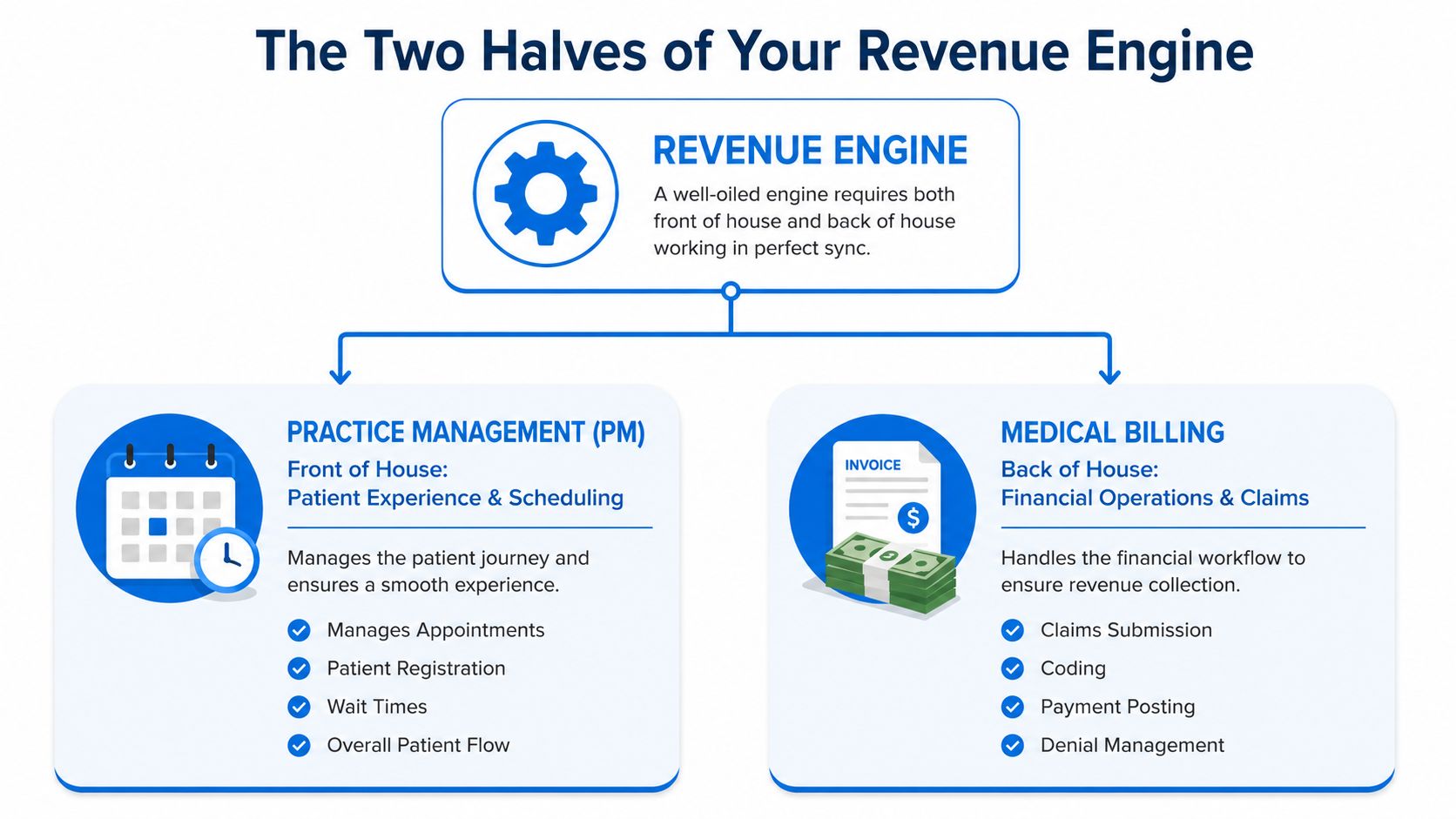
Practice management runs the front end
Your patient flow and financial data start here. Scheduling, registration, insurance capture, benefit checks, referral tracking, authorization workflows, provider calendars, and patient communications all live here.
When this side works, the patient arrives eligible, informed, and financially clear. When it fails, the claim is damaged before the visit starts.
Common front-end failures include:
- Bad registration data. A typo in subscriber information can derail the claim later.
- Weak eligibility checks. Staff confirm a card exists, but not whether coverage applies to that date and service.
- Missed authorizations. The visit happens, but payment never follows.
- Poor patient balance workflow. Staff avoid financial conversations, so collectible balances age immediately.
Medical billing protects the back end
Once care is delivered, billing takes over. Coding, charge capture, claim creation, claim submission, payment posting, denial follow-up, appeals, and patient statements all sit here.
Billing doesn't create revenue out of thin air. It converts operational accuracy into collectible dollars. If your front office enters bad data, your billers inherit a mess. If your clinicians document poorly, coders either undercode, overcode, or stop to chase clarifications.
A denied claim is often just a scheduling error that showed up later wearing a billing costume.
They only work as one system
Many CEOs get trapped when they try to fix the back end without repairing the front end.
That's backwards. If the scheduler collects the wrong insurance, the biller can't rescue the claim with heroics. If the authorization team misses a requirement, the denial team is stuck arguing from a weak position. If the provider note doesn't support the code, collections won't repair the documentation gap after the fact.
Use this simple test. When a denial comes in, ask one question first: Where did this problem start? Not who touched it last. Where did it start?
That question changes leadership behavior. It shifts the focus from blame to process design.
Your Revenue Cycle From Patient to Payment
Most CEOs see revenue cycle management as claim submission plus collections. That's too narrow. The revenue cycle starts before the patient walks in and ends only when every legitimate dollar is collected, adjusted, or resolved.
This visual lays out the full path.
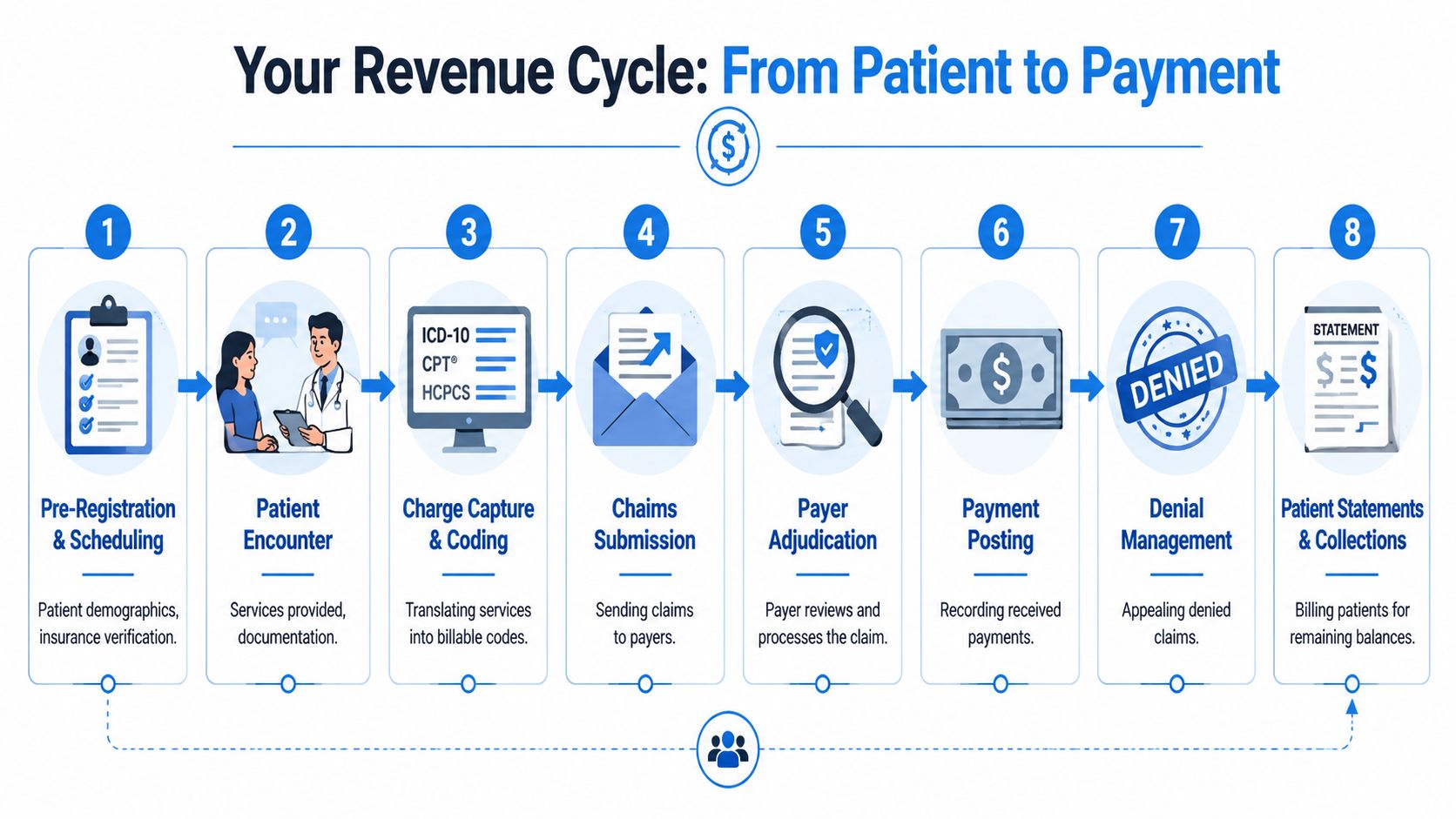
Pre-visit work decides whether you get paid
The first stage is operational, but it's also financial. Someone schedules the visit. Staff collect demographics, insurance details, and the reason for the visit. Eligibility gets checked. Referrals or prior authorizations get secured when needed. Patient responsibility is estimated and communicated.
If your team skips rigor here, the rest of the cycle becomes rework.
A useful reference is this healthcare revenue cycle flowchart, because it shows what executives often miss. The data collected before the visit determines whether the claim can move cleanly after the visit.
The encounter creates the billable story
During the visit, the clinician provides care and documents it. That note isn't just a clinical record. It's the legal and financial basis for coding and reimbursement.
Weak notes create three bad choices:
- Undercode the visit and leave money on the table.
- Code aggressively and increase audit risk.
- Send queries back to providers and slow throughput.
Charge capture also matters here. If services, supplies, or procedures aren't captured correctly, there's nothing for billing to recover later. Revenue you never billed is gone.
Here's a quick executive view of where risk concentrates:
| Stage | What must be right | What breaks if it isn't |
|---|---|---|
| Scheduling | Patient and payer data | Eligibility failures, wrong payer routing |
| Pre-service clearance | Authorization and referral requirements | Avoidable denials |
| Encounter | Documentation specificity | Coding disputes, downcoding |
| Charge entry | Complete services captured | Missed revenue |
| Claim creation | Accurate codes and modifiers | Rejections, denials |
A short explainer can help non-billing leaders see the flow in action.
The back end either protects revenue or leaks it
After coding, claims go out. Payers adjudicate. Payments come back. Then comes the stage many practices undervalue: payment posting.
Posting isn't data entry. It's contract enforcement.
Practices lose up to 5 to 10% of revenue because underpayments go unchallenged when staff lack contract-specific frameworks, according to UnisLink's analysis of how medical practices lose money. If your team posts what came in without comparing it to the fee schedule and payer terms, you train the payer to keep paying less.
Payment posting should answer two questions: what did we receive, and was it correct?
Then come denials, appeals, patient statements, and final collections. Many executives focus on these because the pain is visible. But by then, you're dealing with symptoms. The cause usually sits upstream in workflow design, data discipline, or documentation habits.
Why Revenue Leaks and Compliance Risks Emerge
A denied claim feels like a payer event. Usually it's an internal process event that surfaced late.
That distinction matters because cash problems rarely start in billing alone. They start when front-desk workflows, clinical documentation, coding, posting, and follow-up operate like separate departments instead of one revenue engine. The handoff breaks. Revenue breaks with it.
Revenue leakage starts upstream
New practice leaders often look at denials, aging AR, or patient complaints and assume the business office needs to work harder. Usually the business office is cleaning up damage created earlier.
A registration typo can trigger an eligibility mismatch. A missing authorization can turn a valid visit into a denial. A thin note can force coding down or make an appeal unwinnable. A payment posted without checking contract terms can hide underpayments for months.
Those are not isolated billing mistakes. They are operating failures with financial consequences.
Every front-end shortcut shows up later as back-end rework, delayed cash, or lost revenue.
The patterns are predictable:
- Registration errors create demographic and insurance mismatches
- Missing authorizations leave high-value services exposed
- Documentation gaps produce unsupported codes and weak appeals
- Slow follow-up turns recoverable claims into write-offs
- Unworked underpayments let payer errors pass as normal reimbursement
If you want fewer denials, fix intake, documentation, and ownership first. Denial management alone is a mop. Workflow discipline is the roof repair.
Rework is expensive, even when the claim gets paid
A broken process forces your staff to touch the same dollar multiple times. They correct claims, request addenda, call payers, resend records, and answer patient balance complaints that should never have existed.
That labor is pure recovery cost. It does not produce new revenue. It just tries to salvage revenue your operation already damaged.
For a CEO, the warning signs are familiar:
- AR stays open too long
- Staff spend too much time on corrections
- Cash collections swing month to month
- Patient statements create confusion and calls
- Managers struggle to explain why production and deposits don't match
This is why billing and practice management should be run as one system. Scheduling, registration, documentation, coding, and collections all feed the same financial result. If one step is weak, the rest of the cycle absorbs the cost.
Compliance risk follows the same workflow failures
Compliance problems also begin in daily operations.
When registration is rushed, identity, consent, and privacy steps get missed. When documentation habits drift, coding accuracy drifts with them. When staff roles are unclear, no one catches missing signatures, unsupported services, or payer-specific requirements before the claim goes out.
Policy binders do not prevent that. Process control does.
Strong practices build checkpoints into the workflow:
- Eligibility and benefit verification before service
- Clear authorization ownership before scheduled care
- Documentation standards tied to coding requirements
- Payment posting that checks contract accuracy
- Assigned accountability for denials, appeals, and patient balances
If your net collection rate is weak, this is usually where the damage starts. The claim may fail at the back end, but the leak often began at the front end.
That is the central mistake practices make. They treat medical billing and practice management as two functions. They are one financial engine. Run them that way, and you reduce denials, protect compliance, and get cash in the door faster.
Measuring the Financial Health of Your Practice
Practices can stay busy, see full schedules, and still bleed cash. The fix is not more reporting. It is better reporting tied to the workflow that created the result.
You need a short dashboard that shows whether your front desk, clinical team, coding, and follow-up are producing collectible revenue or creating expensive rework.
The first metric to watch is Net Collection Ratio. It answers the question that matters most. After contractual adjustments, how much of the money your practice earned did you collect?
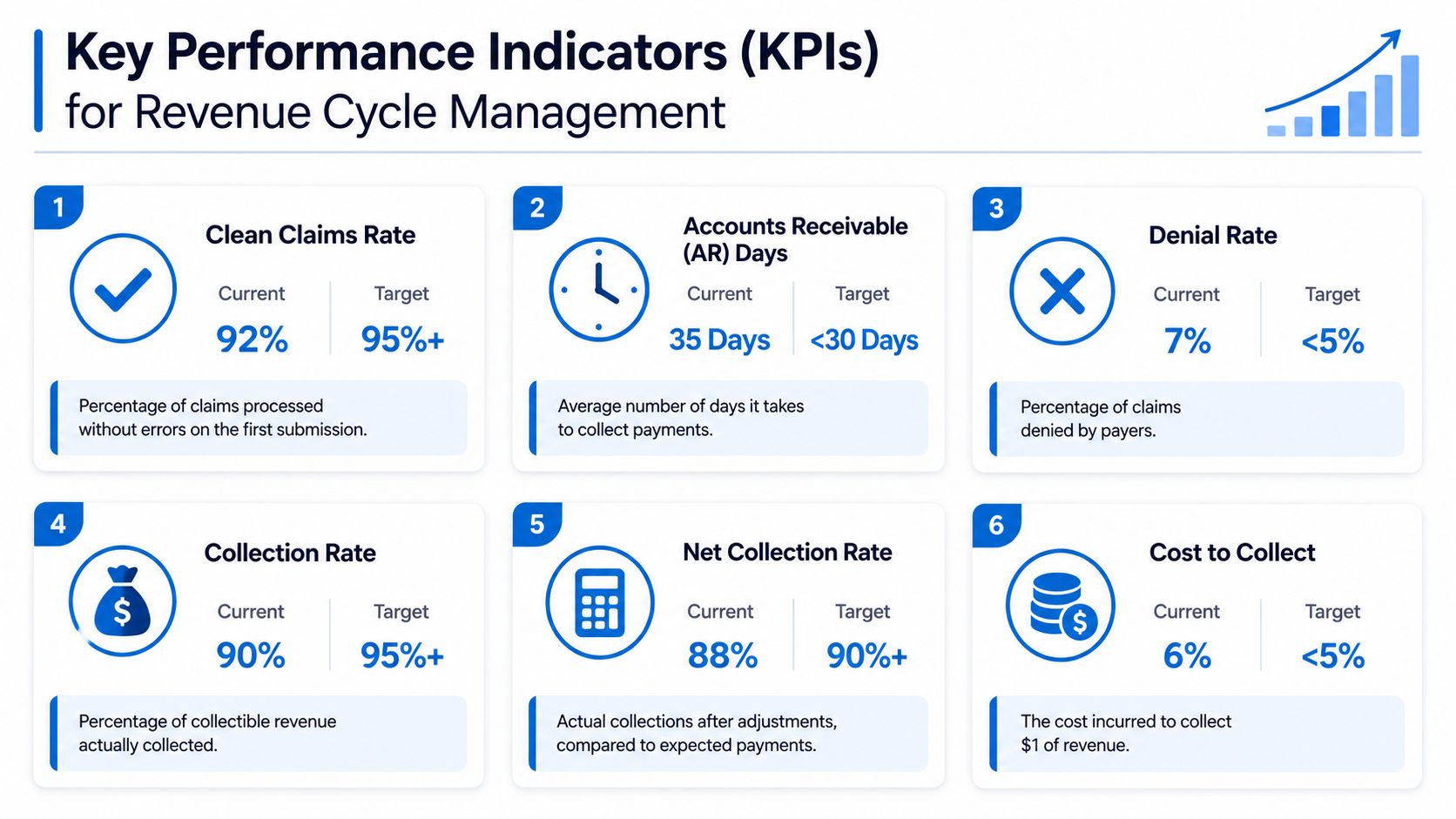
Net collection ratio tells you if your system works
High-performing practices achieve a Net Collection Ratio of 96 to 97% and keep Claims Denial Rate below 8%, according to MGMA benchmark figures summarized by ProMD Medical Billing.
If your NCR is below that range, do not blame the billing office first. Low collections often start much earlier. Eligibility was not verified. Authorization was missed. Documentation did not support the code. The claim reached billing already damaged.
That is why this metric matters so much. It measures the output of the whole operating system, not just the collections team. For a plain-English explanation of the metric itself, review this guide to how net collection rate measures collectible revenue performance.
Denial rate and days in AR show where cash gets stuck
Denial rate is a rework meter. When it rises, your staff is doing the same job twice, sometimes three times. That slows cash, increases labor cost, and creates write-off risk.
Days in AR measures speed. The same benchmark data points to a 45-day target. If your AR runs long, cash is trapped somewhere in the workflow. Usually the problem is not mysterious. Claims are sitting for missing information, denials are aging without action, payment posting is incomplete, or patient balances are not being worked consistently.
Those are management problems, not reporting problems.
Build an executive dashboard your team can act on
Keep the dashboard short. Review it on a fixed cadence. Assign one owner to each metric, because a KPI without an owner is just decoration.
A practical dashboard looks like this:
| KPI | What it tells you | What a bad number usually means |
|---|---|---|
| Net Collection Ratio | Whether you collected what was actually owed | Revenue leakage, weak front-end controls, poor follow-up |
| Claims Denial Rate | How often payers are rejecting work | Eligibility, authorization, coding, or documentation breakdowns |
| Days in AR | How quickly revenue turns into cash | Backlogs, rework, slow follow-up, unresolved balances |
| First-pass performance | Whether claims go out cleanly | Weak data discipline at intake or coding |
Ask one hard question in every leadership meeting: if a KPI worsens, can the responsible leader name the root cause, the workflow step involved, and the corrective action in five minutes?
If the answer is no, your practice is still treating operations and billing as separate functions. They are one financial engine. Measure them that way.
Deciding Between In-House and Outsourced RCM
This decision is strategic, not administrative. You're choosing how the practice will build capability, manage risk, and scale operations.
The wrong choice creates overhead, weak accountability, and finger-pointing. The right choice gives you clear ownership and stable collections.
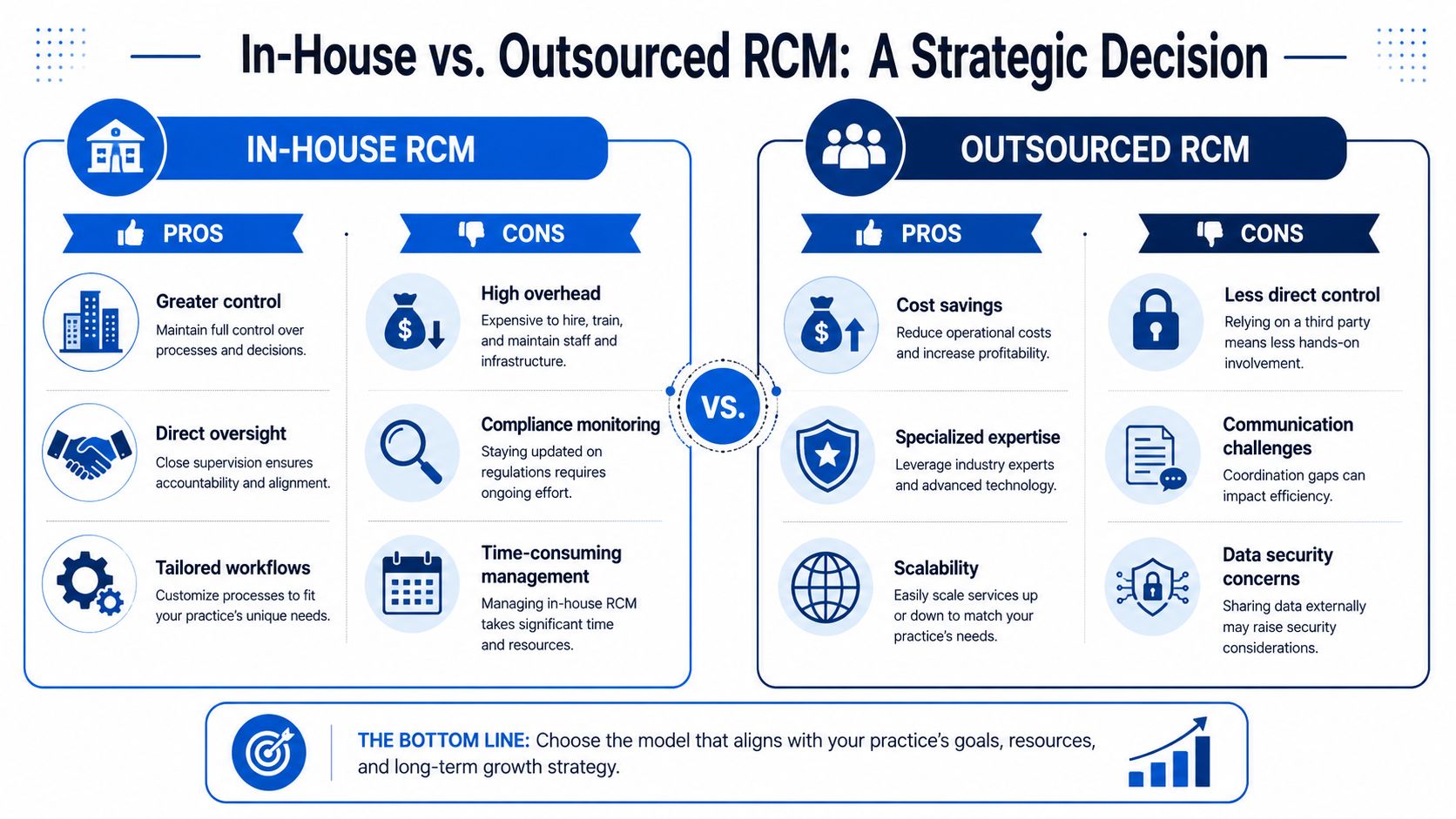
When in-house makes sense
An in-house team can work well if you want direct control over staff, workflows, and communication with providers. It can be the right model when the practice has strong operational leadership and enough scale to support specialized roles.
The advantages are real:
- Closer clinical alignment. Billers can resolve documentation questions quickly.
- Direct oversight. Leaders can see bottlenecks without waiting on a vendor queue.
- Workflow customization. You can design processes around specialty-specific habits and provider preferences.
But in-house RCM only works when management is disciplined. Otherwise, you end up with a few overextended employees carrying payer rules, appeal logic, posting, and patient collections in their heads. That's fragile.
When outsourcing makes sense
Outsourcing makes sense when you need expertise, coverage, or process depth you don't have internally. It also helps when growth outpaces your ability to hire and train.
A capable partner should bring:
- Operational specialization across denials, payment posting, and payer follow-up
- Process consistency so work happens on schedule, not when one key employee has time
- Scalability when volumes shift
- Reporting discipline that many small internal teams never build
Some practices choose a full-service model. Others keep selected functions close to the clinic and outsource the rest. For example, Clarity's medical billing services support both full-cycle and customized operating models, which is often a better fit than forcing every function into one setup.
The hidden outsourcing risk is siloing
Most outsourcing advice misses the main trap. It's not merely loss of control. It's functional siloing.
Data shows 30 to 40% of denial recovery failures stem from misaligned handoffs between outsourced teams and in-house clinical staff, according to OmniMD's discussion of improving practice revenue. That happens when one group owns denials, another owns authorizations, providers control documentation, and nobody shares a common operating rhythm.
If you outsource, don't split the work in ways that break accountability.
Use this checklist before signing anything:
| Decision point | Healthy model | Bad model |
|---|---|---|
| Ownership | One named owner for each handoff | Shared responsibility with no final decision-maker |
| SLA design | Timelines tied to clinic workflow | Timelines tied only to vendor queue |
| Denial feedback | Trends sent back to scheduling and clinical teams | Denials worked in isolation |
| Escalation | Provider questions resolved quickly | Documentation issues bounce for days |
The point isn't in-house versus outsourced. The point is whether the model preserves operational continuity.
How to Choose the Right RCM Partner
Don't shop for a vendor that “does billing.” Shop for a partner that can diagnose where your revenue engine is failing.
A real evaluation starts with your bottleneck. Are denials climbing because authorizations are weak? Are payments being posted without contract review? Are patient balances aging because front-desk collection habits are inconsistent? If you don't define the operational problem first, every sales pitch will sound fine.
Ask operational questions not sales questions
You need specifics, not slogans.
Ask questions like:
- How do you handle eligibility and authorization failures before claims go out?
- What does your payment posting process do beyond recording cash?
- How do you route denial trends back to scheduling, coding, and clinical teams?
- What reporting will show root causes, not just totals?
- Can you support only the functions we need, or do you require a full handoff?
A weak partner talks about software and dashboards. A strong one talks about work queues, ownership, escalation rules, and handoffs.
Choose the team that can explain how a scheduling mistake turns into a denial, and how they'd stop it from happening again.
Demand reporting you can act on
Reporting should help you decide, not just observe.
Good reporting shows patterns by payer, denial category, work queue, and operational source. It should let you answer practical questions fast. Which denials came from missing auths? Which balances are collectible but untouched? Which provider workflows generate coding delays? Which payers are paying below contract terms?
If a report can't lead to an action item, it's decoration.
Choose a partner model that fits your bottleneck
Not every practice needs a full outsource. Some need help with payment posting and underpayment review. Others need benefit verification discipline. Others need denial cleanup while rebuilding front-end operations internally.
Pick the model that matches your operational reality:
- Full-service support when internal infrastructure is thin
- A la carte support when one or two functions are dragging down the rest
- Transitional support when you're rebuilding process and staffing
The right RCM partner should improve control, not remove it. They should make your workflow more visible, your accountability sharper, and your financial performance easier to manage.
Clarity offers complimentary revenue cycle consultations for practices that need a clearer view of where billing and operational workflows are hurting cash flow. If your team is dealing with denials, inconsistent payment posting, weak verification, or fragmented handoffs, a focused review can identify where the process is breaking and whether full-service or targeted support makes more sense.
No responses yet