Monday starts with a full schedule. By Wednesday, your billing manager is chasing missing authorizations, coders are holding charts, physicians are asking why cash is tight again, and the front desk is fielding calls from patients who don't understand their statements. Nothing looks catastrophic in isolation. Together, it feels like the practice is working hard and getting paid late.
That's the trap. Most leadership teams experience revenue cycle problems as scattered annoyances: a denied claim here, an aging balance there, a staff member who's clearly exhausted, a patient who gives up halfway through a payment conversation. But those aren't separate issues. They're signals from the same operating system.
Revenue cycle management for healthcare providers is that operating system. It governs whether the care you deliver turns into clean claims, timely payment, and predictable cash flow. When it runs well, your organization has room to invest in staff, technology, and patient experience. When it runs poorly, every department feels it.

Table of Contents
- Why Your Practice's Financial Health Depends on RCM
- The Seven Stages of Your Revenue Cycle Journey
- The Financial Vital Signs You Must Track
- Diagnosing Your Practice's Revenue Leaks
- How to Streamline RCM for Maximum Profitability
- In-House vs Outsourced RCM A Strategic Decision Framework
- Taking Control of Your Practice's Financial Future
Why Your Practice's Financial Health Depends on RCM
Monday starts with a full clinic, but by Friday the leadership team is asking a familiar question: why does cash still feel tight? If appointments are strong, providers are productive, and demand is steady, the gap usually sits in revenue cycle execution.
RCM works like the wiring behind the walls of a practice. Patients do not see it, but every registration error, missing authorization, coding gap, delayed claim, and unanswered denial affects whether care delivered turns into cash collected. In finance terms, it is the difference between booked revenue and usable revenue.
That distinction matters more than many leaders realize. A busy schedule can hide weak collections for months. Teams keep working harder, physicians see more patients, and managers chase yesterday's problems. Then the symptoms show up in places that feel operational at first: front-desk stress, coding backlogs, old AR, more patient billing calls, and less confidence in the numbers discussed at month-end.
RCM is where operational friction turns into margin loss
A rushed eligibility check does not stay a front-desk problem. It becomes a denied claim, then a reworked account, then a later patient bill, then a harder collection conversation. The cost is not only delayed cash. It is staff time, avoidable overtime, and frustration that spreads across the practice.
That is why I advise leadership teams to treat RCM as a working capital system, not a billing task. If cash is inconsistent, the practice usually has one of two problems. It is either failing to capture revenue it earned, or collecting it too slowly to support payroll, hiring, and growth without constant pressure.
A simple way to assess this is to map the handoffs from scheduling to final payment. A clear healthcare revenue cycle flowchart for medical practices helps leaders see where revenue stalls, where staff rework piles up, and where patient experience breaks down.
Practical rule: If staff spend large parts of the day fixing preventable errors, the revenue cycle is already draining margin.
What strong RCM looks like in practice
Strong RCM rarely looks dramatic. It looks controlled.
- Accurate intake: Insurance, demographics, and coverage details are verified before the visit whenever possible.
- Usable documentation: Providers document clearly enough for coding and billing teams to act without repeated clarification.
- Fast exception management: Denials, underpayments, and missing information are worked quickly before they age into harder collections.
- Clear patient balances: Statements and payment expectations are understandable, so patients can respond without confusion.
The financial effect is straightforward. Fewer errors mean fewer touches per claim. Fewer touches lower labor cost. Faster, cleaner claims improve days in AR and reduce the need for staff to spend their day on recovery work instead of prevention.
Practices with steady cash flow do not get there through heroic effort. They get there through disciplined process, clear ownership, and smart decisions about which parts of RCM should stay in-house and which should be outsourced.
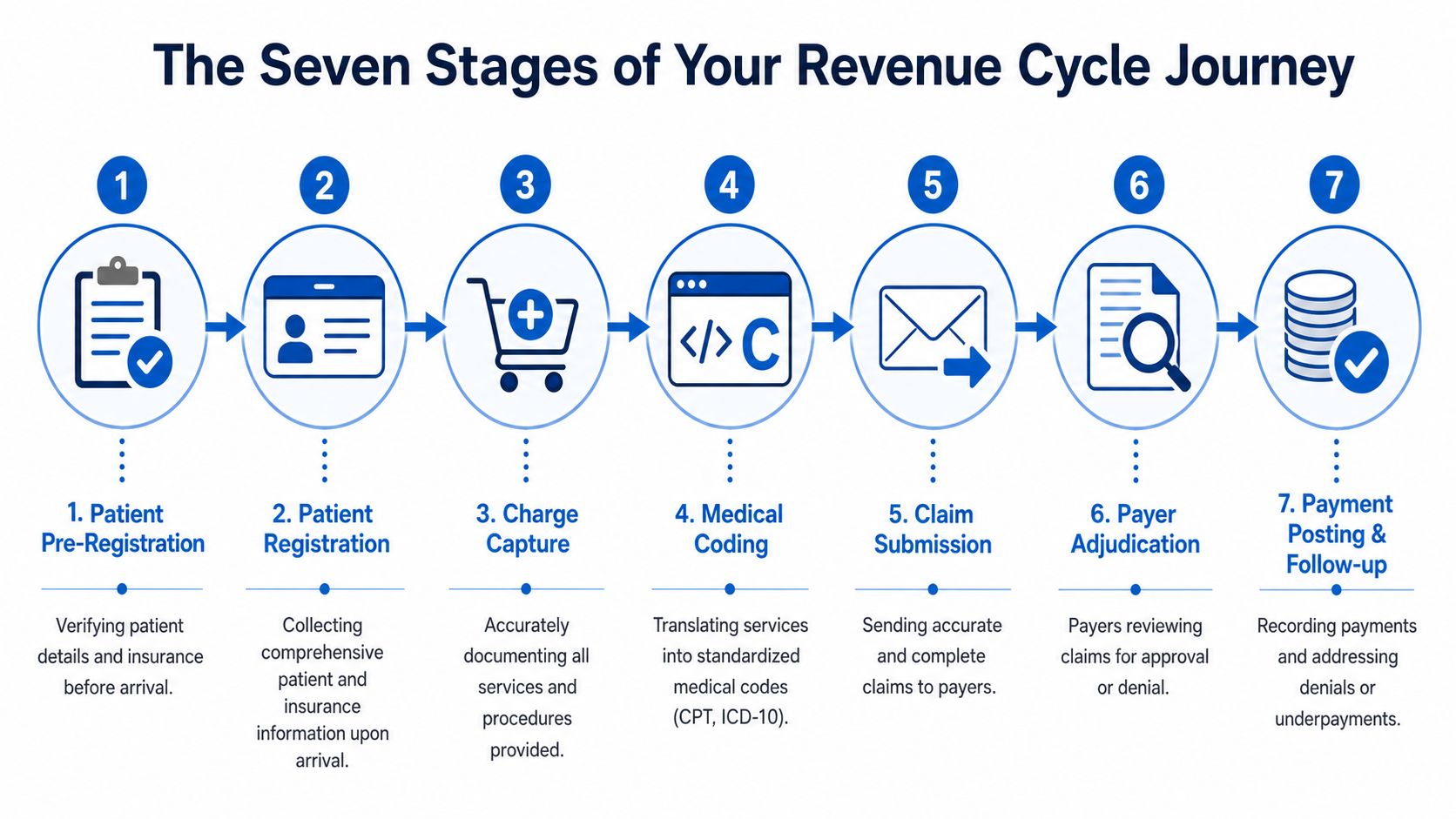
The Seven Stages of Your Revenue Cycle Journey
Monday starts with a full schedule, but the week's cash position may have already been decided before the first patient arrives. An eligibility miss at 8:00 a.m., incomplete documentation at noon, and a claim edit at 4:30 p.m. can turn a productive clinic day into delayed revenue, avoidable rework, and frustrated staff.
The revenue cycle works like a chain of financial custody. Each handoff either protects margin or puts it at risk.
RCM works like a relay race
RCM works like a relay race. Early mistakes travel downstream and get more expensive to fix. A front-desk error that takes 30 seconds to prevent can take billing staff weeks to correct after a denial, and by then the patient may also be confused about what they owe.
Patient pre-registration and eligibility verification
Coverage, benefits, authorization requirements, and patient responsibility should be confirmed before the visit when possible. This is the first cash control point. If the practice starts with bad insurance data, every later stage costs more labor.Patient registration
At check-in, staff confirm demographics, insurance details, and guarantor information. Registration accuracy affects more than claim acceptance. It also shapes the patient's financial experience, because bad data often leads to wrong statements, repeated calls, and avoidable collection friction.Charge capture
Every billable service has to be recorded completely and quickly. Missed charges are quiet revenue loss. They do not trigger the same urgency as denials, but they reduce earned revenue just as directly.Medical coding
Coding converts documentation into the language payers use to decide payment. The trade-off is constant. Teams need speed, but speed without accuracy increases denials, compliance risk, and underpayment.
A shared process map helps leaders see where accountability sits and where work stalls between teams. This healthcare revenue cycle flowchart for medical practices makes the connection between front-end intake, mid-cycle documentation and coding, and back-end collections easier to spot.
After the encounter, the practice finds out whether earlier discipline holds up under payer scrutiny.
Claim submission
Claims are transmitted to the payer with all required data, modifiers, and supporting details. Clean claim performance matters here, but claim submission is usually where upstream problems become visible, not where they begin.Payer adjudication
The payer reviews the claim and decides to pay, reduce, pend, or deny it. This stage tests the quality of everything that came before it. Weak eligibility checks, vague documentation, and coding gaps usually surface here as delayed cash.Payment posting and follow-up
Payments are posted, contractual variances are reviewed, denials are appealed or corrected, and patient balances move into the right workflow. At this stage, leadership can tell whether the operation is collecting what it earned or just staying busy.
Where breakdowns usually happen
RCM has drawn more investment across the industry because practices need tighter control over cash flow, labor costs, and patient collections, as noted earlier. That demand is easy to understand. Every weak handoff increases rework. Rework raises cost to collect, slows cash, and pulls staff away from prevention.
A denied claim is often the final financial result of an earlier operational mistake.
Leaders do not need to master every payer rule. They need a clear view of where money is lost. Registration errors create preventable denials. Incomplete documentation leads to coding delays or unsupported claims. Slow follow-up lets receivables age until recovery rates drop and staff burnout rises.
A healthy revenue cycle is not a billing department goal alone. It is the operating system for the practice's financial health.
The Financial Vital Signs You Must Track
A practice can stay busy, keep schedules full, and still feel cash pressure every month. The reason is simple. Volume does not equal collected revenue. Leadership needs a short list of metrics that show whether earned revenue is turning into cash without excessive rework, write-offs, or staff strain.

The core dashboard
These four measures usually expose the underlying problem faster than a larger dashboard full of disconnected activity counts.
| KPI | What it tells you | Healthy reading |
|---|---|---|
| Adjusted collection rate | How much collectible revenue you actually collect | 95% to 99% for high-performing practices |
| A/R older than 120 days | How much of your receivables are aging into risk | Ideally below 12% |
| Claim denial rate | How often claims are rejected and forced into rework | Above 10% signals an unhealthy process |
| Cost to collect | How much effort and expense it takes to get paid | Should stay below 10% |
These benchmarks are drawn from Rivet Health's RCM metrics guide and Dean Dorton's healthcare RCM metrics analysis. Break the dashboard down by payer, provider, and location. Otherwise, leadership sees averages that hide the source of the problem.
For teams building reporting discipline, this healthcare revenue cycle analytics resource is a useful reference for structuring operational and financial reporting.
What bad readings usually mean
An adjusted collection rate below target means the practice is delivering care and failing to collect part of the revenue it had a right to earn. The usual causes are unresolved denials, underpayments, inconsistent write-off controls, weak patient balance follow-up, or all four at once. From a finance standpoint, this works like a margin leak. The work is done, the expense is already in the books, and the cash never fully arrives.
A high share of A/R older than 120 days means the receivables balance is losing quality. Older A/R takes more touches to recover, ties up staff who should be preventing new problems, and often produces a false sense of asset value on paper.
Claim denial rate deserves daily attention because it drives both cash delay and labor waste. Once a claim denies, the practice pays twice. First to do the work, then to rework the claim. Dean Dorton's analysis uses 10% as the point where the process is unhealthy. In practice, denials at that level usually trace back to front-end and mid-cycle control failures such as eligibility, coding, and credentialing gaps.
Track trends by month and by payer. A flat month-end total can hide a denial pattern that will hit cash later.
Cost to collect keeps the team honest. A practice can improve collections and still lose ground if it takes too many manual touches, too much overtime, or too much vendor spend to get there. Higher collections with rising collection cost is the financial equivalent of sprinting on a treadmill.
Clean claim rate belongs on the same dashboard even without a benchmark listed here. It shows how often claims leave the system correctly the first time. When that rate drops, productivity often looks busy from the outside while back-office teams burn hours on avoidable corrections.
The goal is not to admire reports. It is to spot which part of the cycle is draining cash, creating patient friction, and overloading staff before the problem grows into a quarter-end surprise.
Diagnosing Your Practice's Revenue Leaks
Leadership teams often focus on the visible symptom. Denials are up. A/R is stretching. Patient balances are sitting longer. Staff say they're overwhelmed. The mistake is treating each one as a separate problem owner.
Most of the time, they're connected.
Symptoms versus causes
A denial is an outcome, not a diagnosis. When a practice sees repeated denials, the root cause usually sits earlier in the chain. Eligibility wasn't verified carefully. Coding lacked specificity. Credentialing details weren't current. Someone corrected the issue once, but nobody fixed the process that produced it.
The same pattern shows up in patient collections. Leadership may blame “self-pay difficulty,” but the deeper problem is often that patients were confused about responsibility before they ever received a statement. When that happens, collections teams inherit a trust problem, not just a balance.
Here's a practical way to frame revenue leakage:
- Front-end leaks: Bad demographics, incomplete insurance details, missed authorizations, unclear patient responsibility.
- Mid-cycle leaks: Weak documentation, coding inconsistencies, missed charges, delayed chart completion.
- Back-end leaks: Slow denial follow-up, payment posting gaps, underpayment review failures, confusing patient statements.
If you only work the back end, you're mopping the floor while the pipe is still leaking.
Two leaks most practices underestimate
The first is staff burnout. Workforce exhaustion directly drives a significant portion of the 80% of denials caused by human error, and it can delay claim submission by 3 to 5 days, according to Medwave's analysis of major RCM challenges. That's not just an HR issue. It's a revenue integrity issue. Tired staff skip steps, make avoidable edits, and stop escalating recurring payer patterns because they're stuck in survival mode.
The second is patient financial literacy. Low patient financial literacy can cause 30% to 40% of patient balance collection failures, increasing A/R days, as discussed in Undue Medical Debt's revenue cycle perspective on health care finances. When patients don't understand estimates, coverage limits, or assistance options, the balance doesn't become more collectible with age. It becomes more disputed.
Burnout and confusion are expensive because they create preventable friction at the exact points where accuracy and trust matter most.
This is why standard RCM troubleshooting often falls short. It looks at denials, but not the exhausted team creating rework. It looks at patient balances, but not the communication failures that turned those balances into bad debt risk. Once you see those links clearly, your improvement plan gets a lot sharper.
How to Streamline RCM for Maximum Profitability
The fastest way to improve margin isn't squeezing one more report out of the billing system. It's reducing avoidable work. Every preventable denial, rebill, correction, and patient complaint adds labor without adding revenue.
That means the best RCM strategy is usually a friction-reduction strategy.
Fix the front end first
If a practice wants faster financial improvement, start before the claim exists.
- Standardize eligibility verification: Use payer portals, automated eligibility tools, and scripting so staff verify the same core items every time.
- Collect cleaner registration data: Tight front-desk workflows beat heroic back-end cleanup.
- Give patients understandable estimates: Plain-language cost conversations reduce surprise and make later collections less adversarial.
- Train for exceptions, not just routine visits: Staff need a playbook for coordination of benefits, authorization-sensitive services, and coverage edge cases.
A lot of leaders instinctively invest in denial work queues first. Those matter, but they don't solve the source of the waste. Prevention pays better than correction.
Build a calmer back office
The back office breaks down when every claim requires custom attention. The goal is to create a system where exceptions are visible and routine work is automated.
Consider this operating model:
| Problem | Better response | Why it works |
|---|---|---|
| Frequent coding edits | Use coding support tools and targeted provider education | Coders spend less time fixing predictable documentation gaps |
| Slow claim release | Add claim scrubbing rules before submission | Errors are caught before they become payer work |
| Denials pile up | Route denials by reason and owner | Teams stop treating every denial the same way |
| Patient collections stall | Simplify statements and offer digital payment options | Patients can understand and act faster |
This is also where staffing design matters. If your experienced billers spend their day correcting minor demographic issues or answering basic balance questions, you've put expensive labor in the wrong seats. Move simple tasks to standard workflows. Reserve specialized staff for appeals, payer variance review, and escalation.
One practical option is a hybrid support model. Some organizations keep patient-facing and provider-facing functions in-house while using outside support for benefit verification, payment posting, denial management, or billing operations. Clarity offers that kind of full-service or a la carte revenue cycle support, which can fit practices that need targeted coverage rather than a total rebuild.
The most profitable revenue cycle isn't the one with the busiest team. It's the one with the fewest avoidable touches per claim.
Technology helps, but only if workflows are clear first. Buying automation on top of confusion just lets a practice move bad data faster. Clean process comes first. Tools accelerate what already works.
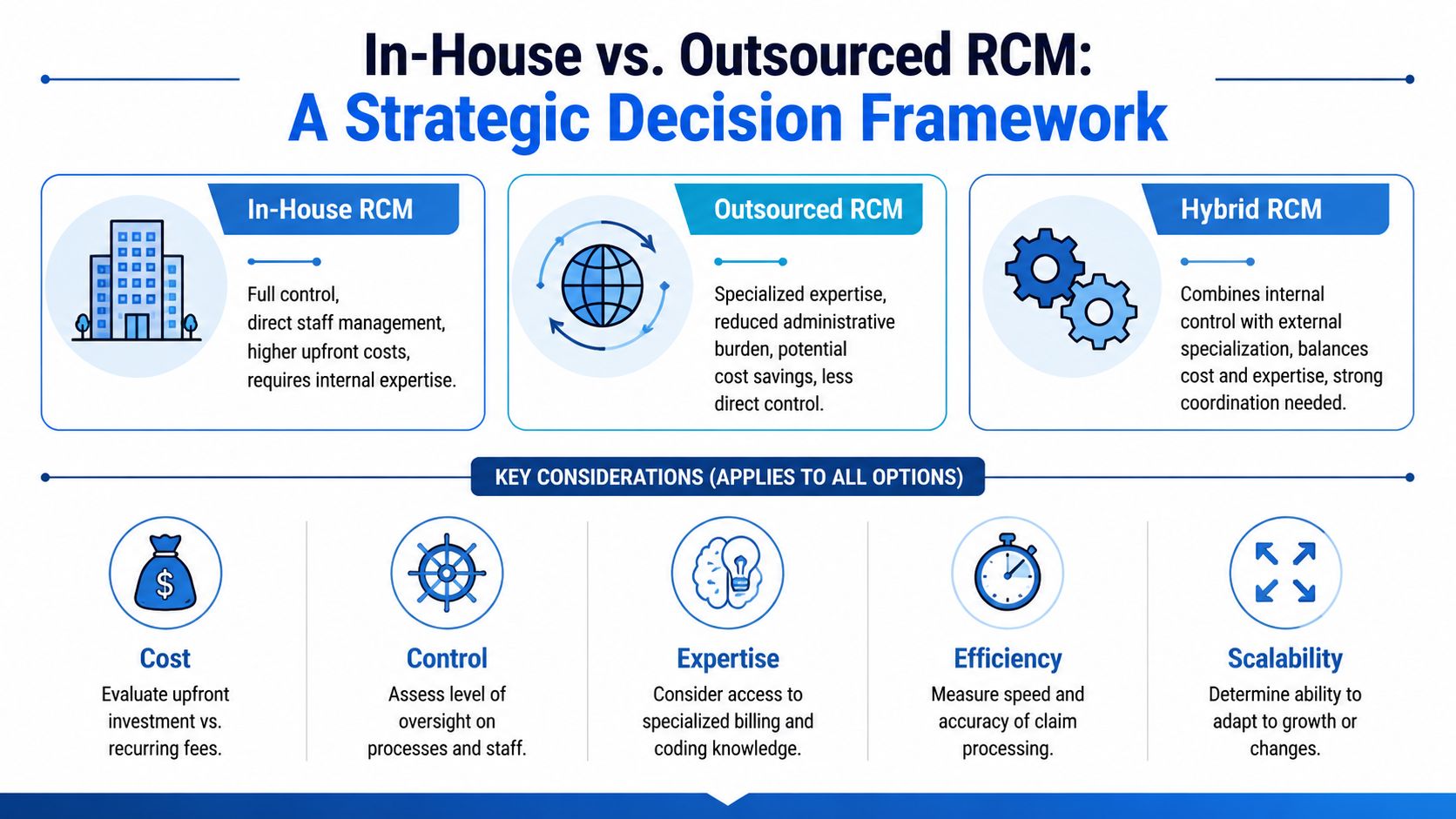
In-House vs Outsourced RCM A Strategic Decision Framework
The in-house versus outsourced debate usually gets framed as control versus cost. That's too simplistic. The actual question is this: where can your organization produce the most reliable financial outcome with the least operational strain?
When in-house makes sense
Keeping RCM in-house can work well when the practice has stable leadership, low turnover, strong specialty knowledge, and disciplined reporting. It also helps when providers want close operational visibility and can support the talent, training, and systems required.
In-house teams usually perform best when:
- The specialty is highly nuanced: Internal coders and billers are intimately familiar with the documentation patterns and payer quirks.
- Leadership reviews KPIs consistently: Problems get caught early instead of aging into large cleanup projects.
- Processes are already documented: New hires can step into a system, not invent one.
The hidden risk is fragility. If one experienced biller leaves and nobody else understands a payer workflow, performance can slide quickly.
When outsourcing is the smarter move
Outsourcing makes sense when a practice needs specialized knowledge, steadier execution, or relief from staffing pressure. It's often the right move when denial management is inconsistent, payment posting lags, or leaders know they need tighter process but don't want to build every capability internally.
This medical billing services overview is useful as a baseline for understanding what outsourced support can cover across daily billing operations.
A hybrid model often works best in practice. The practice keeps the tasks that benefit from proximity, such as patient-facing intake or provider documentation coaching, and outsources functions that require concentrated expertise or heavy follow-up.
A practical evaluation checklist
Use a decision lens that goes beyond vendor promises.
| Decision factor | In-house | Outsourced | Hybrid |
|---|---|---|---|
| Control | Highest direct oversight | Less day-to-day visibility | Shared oversight |
| Expertise access | Depends on hiring success | Broader specialty support | Targeted external depth |
| Scalability | Slower to expand | Easier to add capacity | Flexible if coordinated well |
| Management burden | Highest | Lower internal burden | Moderate |
| Process consistency | Varies by internal discipline | Depends on partner governance | Depends on handoff quality |
When evaluating a partner, ask for specifics:
- Reporting transparency: What dashboards do they provide, and how often?
- Specialty alignment: Have they worked in your clinical and payer environment?
- Workflow ownership: Who handles denials, variance review, and unresolved claims?
- Technology stack: How do they integrate with your EHR, PM, and clearinghouse workflows?
- Compliance discipline: How do they document processes, permissions, and audit readiness?
A good decision framework doesn't ask, “Should we outsource?” It asks, “Which model gives us the strongest control over cash, accuracy, and staff load?”
Taking Control of Your Practice's Financial Future
Revenue cycle management for healthcare providers isn't a mystery and it isn't just an administrative necessity. It's a measurable operating system that determines whether your practice turns clinical work into dependable revenue. When leadership treats denials, aging A/R, staff burnout, and patient confusion as connected signals, the path forward becomes clearer.
The practical move is to diagnose before you redesign. Review where revenue is leaking, which tasks are creating avoidable rework, and whether your current team structure can realistically support better performance. Then decide what to fix internally, what to automate, and what to hand off.
Practices don't need more noise around RCM. They need financial clarity, cleaner workflows, and a system that supports patient care instead of distracting from it.
If you want a clearer view of where your revenue cycle is helping or hurting the practice, Clarity offers a complimentary consultation of your current RCM process. It's a practical first step for identifying workflow gaps, deciding what should stay in-house versus outsourced, and building a plan around better efficiency, accuracy, and profitability.
No responses yet