The U.S. revenue cycle management market reached USD 172.24 billion in 2024 and is projected to grow at a 10.1% CAGR from 2025 to 2030, according to Grand View Research's U.S. RCM market analysis. That should change how you think about your revenue cycle management team.
This isn't a back-office billing function. It's the mechanism that decides whether your clinical work becomes cash, delay, write-off, or bad debt. A weak team turns strong patient volume into financial instability. A disciplined team protects margin, supports hiring, and gives leadership room to invest in growth instead of chasing missing payments.
Most organizations still make the same mistake. They debate headcount and job titles before they decide what operating model produces the best financial return. That's backwards. The right question isn't “Who do we need?” It's “What team structure gives us the most control over collections, denials, speed, and cost?”
Table of Contents
- Why Your Revenue Cycle Management Team Is a Profit Center
- Anatomy of a High-Performing RCM Team
- Key Roles and Core Responsibilities on the Team
- Mapping the RCM Process and Critical KPIs
- Overcoming Common RCM Pain Points with Technology
- Choosing Your RCM Team Model Insource Hybrid or Outsource
- Building a Financially Resilient Healthcare Practice
Why Your Revenue Cycle Management Team Is a Profit Center

A revenue cycle management team is a profit center because it controls the conversion of care into collectible revenue. Clinical volume creates opportunity. RCM determines how much of that opportunity turns into cash, how fast it arrives, and how much margin gets lost to avoidable rework.
That distinction matters more than many owners and CFOs admit. A weak team does not just create billing headaches. It raises labor cost, delays cash, inflates write-offs, and forces leadership to solve revenue problems by adding more visits instead of fixing collection yield.
Two organizations can deliver the same care to the same payer mix and post very different financial results.
The difference is rarely luck.
One group treats RCM like back-office administration. Front-desk errors flow downstream. Claims go out with defects. Denials pile up. Staff spend their day fixing preventable mistakes. Cash becomes unpredictable, and leadership responds by pushing providers harder.
The stronger group treats RCM like an operating asset. It builds controls at the front end, catches errors before claim submission, and assigns follow-up work based on dollar value and payer behavior. That team protects margin the way supply chain protects inventory. It prevents revenue leakage before finance has to explain it.
Your RCM team works like the financial gearbox of the organization. If it slips, the engine revs, labor increases, and cash still does not move.
Profit-center thinking changes how you make staffing decisions. You stop asking whether billing is “covered” and start asking which team structure produces the best return. Can your in-house team collect faster and with fewer write-offs than a specialist partner? Should you keep patient access and coding close to operations while outsourcing denial follow-up or self-pay collections? Those are investment questions, not clerical ones.
Use a simple test. Judge your RCM model on four outcomes:
- Cash acceleration. How quickly does work move from encounter to payment?
- Yield. How much net collectible revenue do you recover?
- Cost to collect. How much labor, vendor spend, and rework are tied to each dollar collected?
- Control. How clearly can you see performance by payer, location, and staff function?
If your current setup misses targets on those four measures, the team needs redesign, not encouragement. That may mean better front-end staffing, tighter coding oversight, clearer ownership, or a hybrid outsourcing model that improves economics without giving up visibility.
Strong RCM teams do more than support operations. They increase cash reliability, protect margin, and give leadership a cleaner basis for growth decisions.
Anatomy of a High-Performing RCM Team
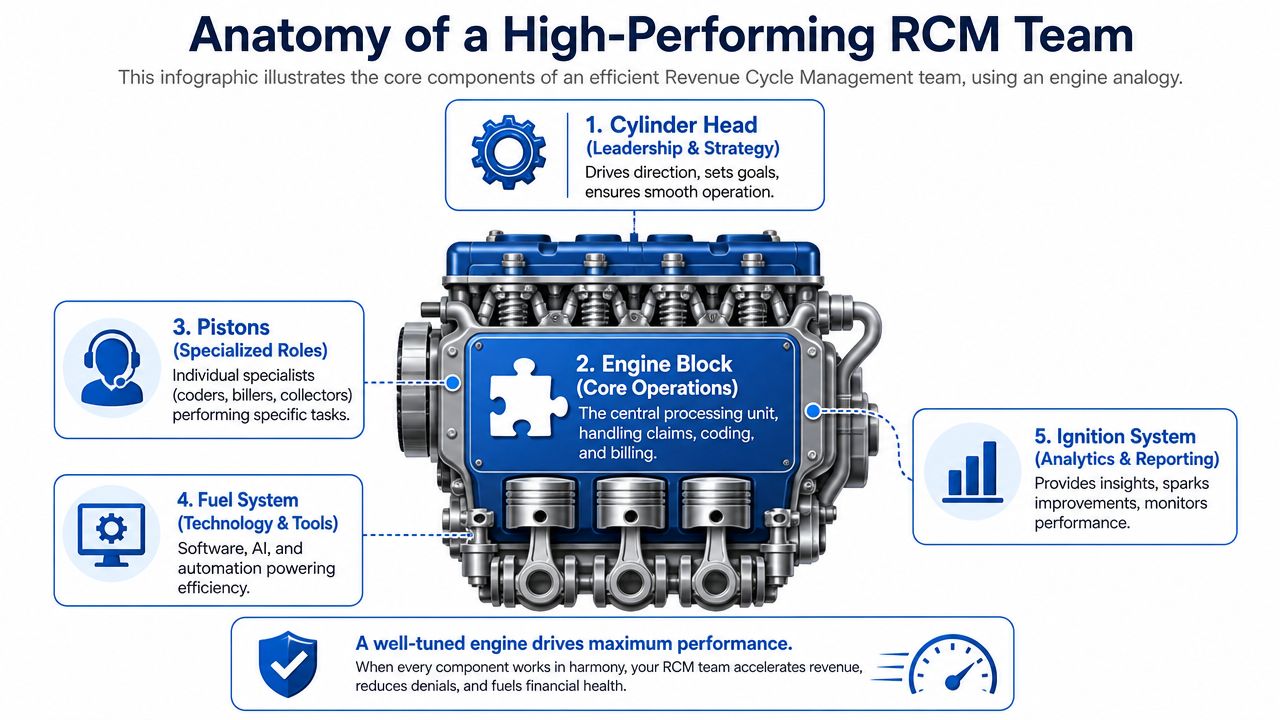
A high-performing revenue cycle management team works like a tuned engine. If one part misfires, the whole machine loses power. You can't compensate for weak intake with heroic denial management any more than you can win a race with a cracked fuel line.
The best teams align people, process, and platforms. Miss one, and the other two spend their time covering mistakes.
People drive accountability
People are still the hardest part. Not because healthcare lacks talent, but because many organizations assign revenue cycle tasks without clear ownership. That creates blind spots. Eligibility gets blamed on coding. Coding blames documentation. Billing blames the payer. Finance blames everyone.
A real team model names accountable operators at each point of the cycle. Someone owns front-end accuracy. Someone owns claim quality. Someone owns payment reconciliation. Someone owns denial trends and escalation.
Process removes friction
Process is the transmission. It decides whether effort turns into movement.
Strong process design does three things:
- Standardizes handoffs so information doesn't get lost between scheduling, coding, billing, and follow-up
- Separates routine work from exception work so specialists spend time on high-value problems, not avoidable cleanup
- Builds controls early because the cheapest denial is the one you prevent before claim submission
Practical rule: If your team fixes the same denial reason repeatedly, you don't have a collections problem. You have a workflow design problem.
Platforms create scale
Technology is the fuel system and dashboard. It powers the engine and tells you when something is wrong. Practice management systems, claim scrubbers, eligibility tools, contract management workflows, reporting dashboards, and automation tools all matter. But tools don't rescue broken operations. They amplify what already exists.
Here's the simplest way to understand it:
| Component | What it does | What happens when it fails |
|---|---|---|
| Leadership and strategy | Sets priorities and enforces accountability | Teams drift and react late |
| Core operations | Executes claims, coding, billing, posting, follow-up | Cash slows and denials rise |
| Specialized roles | Handle skill-based work with precision | Errors spread across the cycle |
| Technology and tools | Reduce manual work and improve consistency | Staff spend time on rework |
| Analytics and reporting | Show where leakage starts | Problems stay hidden too long |
The organizations that outperform don't build a larger engine. They build a coordinated one.
Key Roles and Core Responsibilities on the Team
A revenue cycle management team should be organized by where revenue is won or lost: front end, mid-cycle, and back end. That's more useful than a flat org chart because it ties every role to financial impact.
If you need a broader overview of specialist functions, this breakdown of revenue cycle specialists is a useful reference point. But the issue isn't title inventory. It's operational coverage.
Front-end roles that prevent avoidable loss
The front end is where many organizations leak revenue before a claim even exists.
- Patient access specialist handles registration, demographics, insurance entry, and basic intake accuracy. If this role gets sloppy, denials begin before the visit starts.
- Eligibility and benefits verifier confirms active coverage, payer rules, and plan details. This role protects against claims that should never have been submitted as entered.
- Financial counselor sets patient expectations around responsibility, payment options, and required documentation. Done well, this reduces confusion and strengthens patient collections.
Front-end work is like setting coordinates before takeoff. If the destination data is wrong, the rest of the flight doesn't matter.
Mid-cycle roles that convert services into billable claims
Mid-cycle performance determines whether clinical work is translated accurately into reimbursement.
Medical coder is the translation layer between documentation and claim integrity. When coders work from incomplete notes or inconsistent charge entry, revenue gets distorted fast. Some claims go out undercoded. Others trigger edits or denials.
Charge capture specialist makes sure billable services are recorded completely and routed correctly. This role matters most in environments where documentation, ancillary services, and procedural complexity create room for missed charges.
Billing specialist assembles and submits claims, manages edits, and works rejected claims before they become aging A/R. A billing specialist shouldn't spend the day fixing preventable front-end mistakes. If they do, your labor model is upside down.
Clean billing starts long before claim submission. By the time a claim reaches the billing queue, most of the risk has already been created or removed.
Back-end roles that recover and protect cash
The back end decides whether posted revenue matches expected revenue.
- Payment poster applies payer and patient payments accurately, reconciles adjustments, and flags inconsistencies for review.
- A/R follow-up specialist works unpaid balances, pursues stalled claims, and escalates payer delays before aging turns into write-off pressure.
- Denial management specialist identifies denial patterns, appeals when appropriate, and pushes root-cause fixes upstream.
- RCM manager or director owns reporting, prioritization, staffing decisions, payer issue escalation, and team accountability.
Here's the blunt truth. If you don't have someone explicitly responsible for denial trends and someone else responsible for upstream correction, your team is probably managing symptoms, not performance.
Mapping the RCM Process and Critical KPIs
You can't manage a revenue cycle management team by intuition. You need a process map and a handful of KPIs that expose where cash slows down.
A useful visual reference is this healthcare revenue cycle flowchart. The leadership job is to connect each stage of that flow to a measurable operational signal.
The process from intake to cash
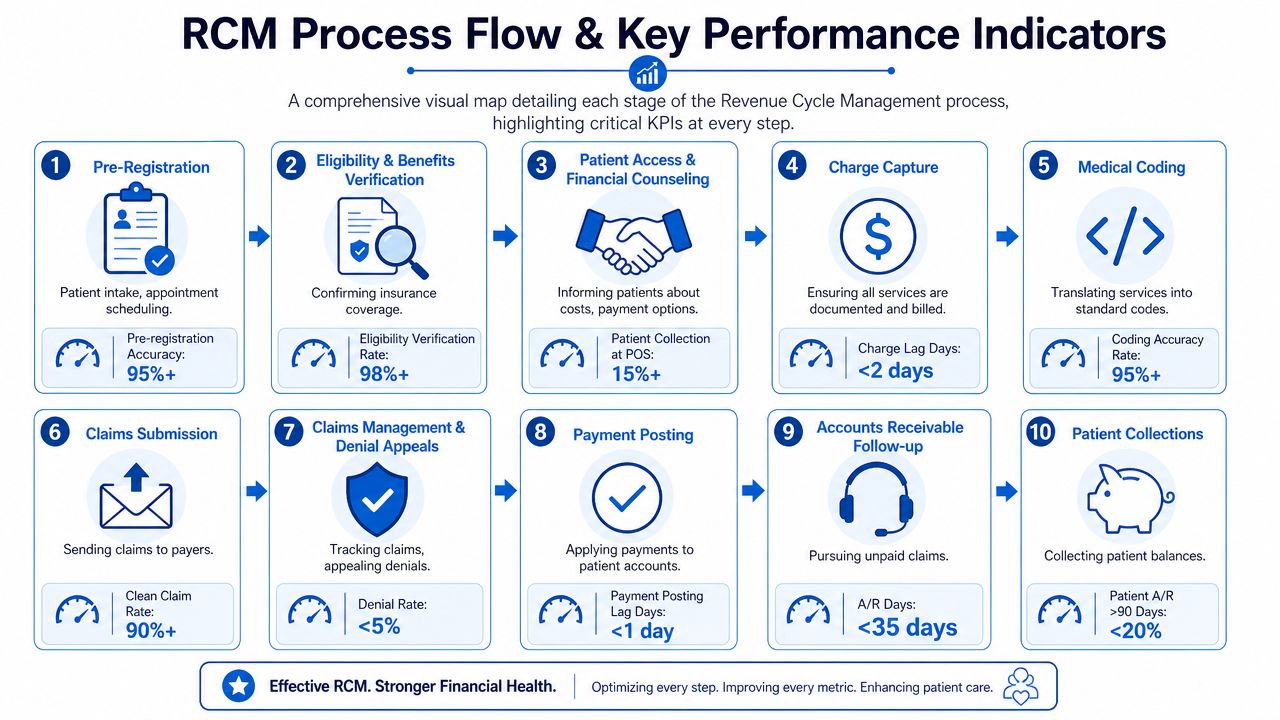
The revenue cycle runs through a predictable sequence:
- Pre-registration and scheduling
- Eligibility and benefits verification
- Patient access and financial counseling
- Charge capture
- Medical coding
- Claim submission
- Claim management and denial handling
- Payment posting
- Accounts receivable follow-up
- Patient collections and reporting
That looks linear on paper. In practice, it behaves more like plumbing. A blockage at the front creates pressure all the way downstream.
The KPIs that matter most
A high-performing revenue cycle management team should center its scorecard on a short set of hard indicators. According to Pharmbills' revenue cycle management metrics overview, a strong team achieves a Clean Claim Rate of at least 95%, with top performers reaching 98%. That same benchmark is tied to a Net Collection Rate of 95% or higher and Days in A/R under 45 days.
Use those numbers as operating thresholds, not vanity metrics.
| KPI | Why it matters | Healthy signal |
|---|---|---|
| Clean Claim Rate | Shows whether claims go out right the first time | At least 95%, top performers 98% |
| Net Collection Rate | Shows how much allowed revenue you actually collect | 95% or higher |
| Days in A/R | Shows how quickly revenue converts to cash | Under 45 days |
What these metrics actually tell you
A low clean claim rate usually points to upstream failure. Registration errors, missing authorizations, weak edits, or coding issues are usually to blame. Don't ask the back end to save a claim that never should have gone out dirty.
Days in A/R tells you whether your process has momentum. If claims age too long, cash gets trapped and management starts making decisions off distorted financial visibility.
Don't overbuild the dashboard. Three well-defined KPIs with weekly accountability beat twenty reports nobody acts on.
Net collection rate is the truth serum. It tells you whether contractual revenue is being collected or leaking away through underpayments, write-offs, avoidable denials, or follow-up failures.
Overcoming Common RCM Pain Points with Technology
Most RCM pain isn't random. It's structural. High turnover, payer complexity, and manual workflows create the same pattern over and over: errors at the front, rework in the middle, aging at the back.
That's why I push leaders to stop framing these as “billing headaches.” They're financial control failures.
Turnover is not just an HR problem
Revenue cycle teams face turnover rates ranging from 11% to 40%, and that instability contributes to denial rates that are often over 10% while pushing Days in A/R beyond the recommended 30 to 45 day range, according to Smarter Tech's RCM statistics review. When experienced staff leave, the organization doesn't just lose labor. It loses judgment, payer pattern recognition, and consistency.
Technology helps by reducing dependence on memory and heroics.
- Eligibility automation catches coverage issues before service or claim submission.
- Claim scrubbers flag common defects before they become denials.
- Automated payment posting shortens the lag between receipt and account reconciliation.
- Work queues and routing rules ensure staff spend time on priority exceptions instead of hunting for tasks.
Use software to standardize, not to decorate
A lot of organizations buy tools and keep the same messy workflow. That doesn't work. Software should simplify decisions, reduce keystrokes, and create visible accountability.
If you're evaluating platforms, start with healthcare RCM software options that support front-end verification, claims management, and payment workflows. Clarity can also function as an operating partner for practices that want end-to-end support or targeted help in selected billing functions. That's one model. Others use a mix of PM systems, clearinghouse tools, and internal analytics stacks.
Good RCM technology acts like guardrails on a mountain road. Staff still drive, but the system prevents expensive mistakes from becoming catastrophic ones.
The strongest technology strategy is boring in the best sense. It removes repeatable manual work, exposes exceptions early, and gives managers enough visibility to coach performance before revenue slips.
Choosing Your RCM Team Model Insource Hybrid or Outsource
This is the decision that matters most. Not whether you need an RCM team. You do. The question is which structure gives you the strongest return on management attention, labor cost, denial control, and cash predictability.
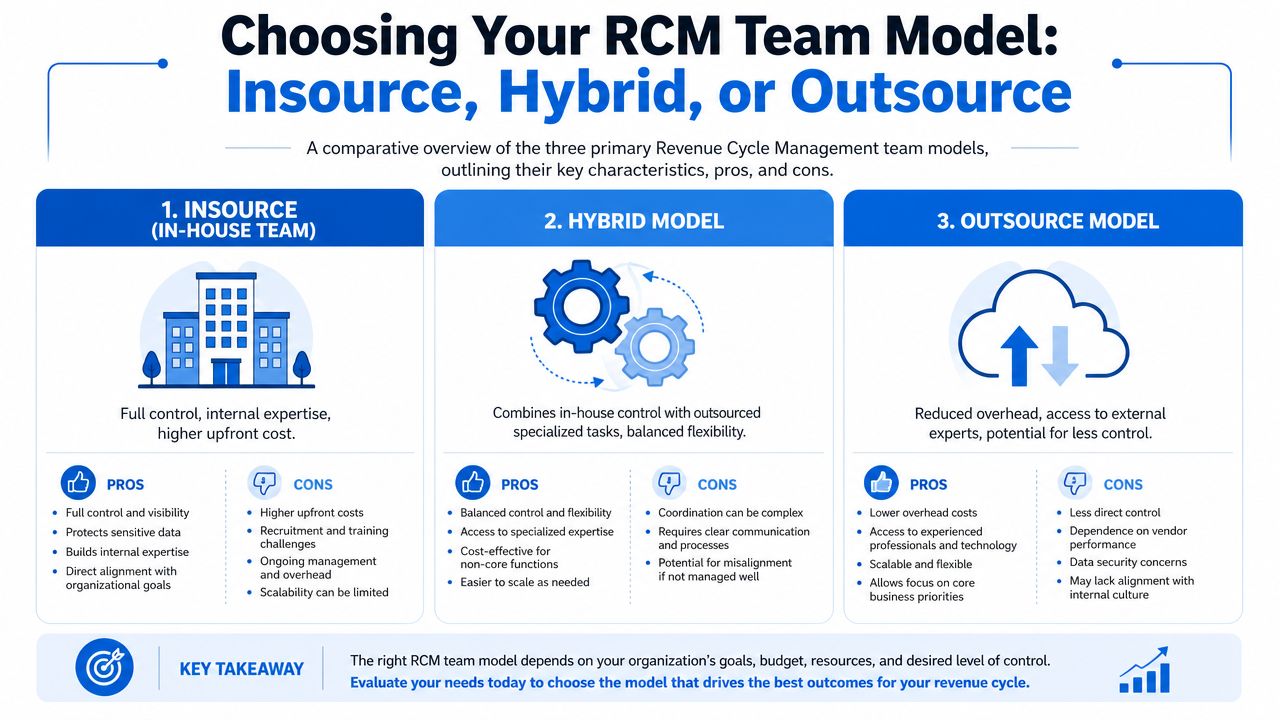
There are three workable models: insourced, hybrid, and outsourced. None is automatically correct. But one of them is usually more economically rational for your organization than the others.
Insource when control is your primary advantage
An in-house revenue cycle management team gives you direct oversight. Leadership can set priorities quickly, align billing with clinical operations, and adapt workflows without vendor coordination. For organizations with stable staffing, disciplined managers, and enough scale to support specialization, insourcing can work well.
The downside is operational fragility. Recruiting, training, absentee coverage, turnover, and technology administration all sit on your balance sheet and management team. If one key manager leaves, performance can slide faster than finance realizes.
Hybrid when you know where your bottlenecks live
The hybrid model is usually the smartest middle ground. Keep strategic control and patient-facing functions internally. Outsource narrow but difficult functions such as coding support, denial management, A/R follow-up, or payment posting when internal capacity is thin or inconsistent.
This model works best when leadership already understands its weak points. If your front end is strong but denial recovery is poor, outsource the recovery function. If your coders are solid but payment posting drags, fill that gap instead of replacing the whole machine.
A hybrid model is the equivalent of keeping the cockpit while hiring a specialist maintenance crew.
Outsource when internal complexity is draining margin
Full outsourcing makes sense when the organization wants scalability, specialized expertise, and less staffing volatility. It can also help when leadership is tired of rebuilding billing teams every year. If your current model depends on a few overextended employees who know “how things work,” you don't have a stable operation. You have institutional luck.
High-performing RCM teams use maturity frameworks to reduce denial rates from over 10% to under 5%, and they routinely monitor payer fee schedules because failure to do so can lead to annual revenue loss of 3% to 7%, according to HFMA's benchmark tool discussion on revenue cycle automation. That matters in this decision because outsourcing only works if the partner brings that discipline, not just labor.
A practical decision framework
Use four filters before you choose a model:
- Control: Do you need daily operational visibility and rapid policy changes?
- Capability: Do you already have strong managers, stable staff, and reliable process discipline?
- Complexity: Are your payer rules, specialties, and denial patterns too specialized for a thin internal team?
- Cost of failure: What happens financially when claims age, underpayments go unnoticed, or denials pile up?
If your current team spends most of its time correcting preventable mistakes, don't ask whether you should add headcount. Ask whether the operating model itself is wrong.
Vendor evaluation checklist
- Reporting transparency: Can the partner show claim status, denial categories, A/R aging, and payment posting detail in a format your finance team can audit?
- Workflow ownership: Who handles eligibility, coding edits, denial appeals, payer follow-up, and patient balances?
- Technology fit: Will the vendor work inside your current PM and EHR stack, or will you inherit new integration problems?
- Escalation discipline: How are payer issues, fee schedule discrepancies, and recurring denial causes identified and escalated?
- Account management: Who owns the relationship, and how often will performance reviews happen?
- Flexibility: Can you outsource only the functions that are broken, or is the arrangement all-or-nothing?
The wrong model creates permanent friction. The right one lets leadership spend less time rescuing collections and more time steering the business.
Building a Financially Resilient Healthcare Practice
A strong revenue cycle management team gives a practice or hospital something every leadership team wants but few build: reliable financial traction. Not perfect collections. Not zero denials. Traction. The ability to turn patient care into predictable cash with fewer surprises and less executive firefighting.
That only happens when team structure matches business reality. Some organizations need an in-house team because control and proximity matter most. Others should use a hybrid model because the smartest move is to protect internal strengths and outsource weak spots. Some should stop pretending they want to run a billing operation at all and move to an outsourced model with tighter oversight.
The common thread is discipline. Define ownership. Map the process. Track the few KPIs that expose leakage. Use technology to reduce preventable work. Then choose the operating model that produces the best financial return, not the model that feels most familiar.
If you're a practice owner, CEO, or CFO, review your current revenue cycle management team like you'd review any major asset. Ask where cash slows down, where labor gets wasted, and where the structure no longer matches the complexity of the work. That exercise usually reveals the answer faster than another staffing debate.
If you want an outside view of where your revenue cycle is leaking cash, Clarity offers a complimentary review of current RCM operations and can support full-cycle management or targeted functions based on your team model.
No responses yet