Margins tighten slowly, then all at once. A few denials linger in work queues. Patient balances age longer than they should. Staff spend time correcting eligibility, reworking claims, and answering billing questions that should've been resolved before the encounter. Leadership sees the symptoms in cash flow, but the underlying problem is usually operational discipline inside the revenue cycle.
That's where revenue cycle specialists matter.
The mistake many hospitals and physician groups make is treating this role as back-office support. It isn't. A strong specialist protects revenue at the points where organizations usually lose it: registration, coverage verification, coding handoff, claim submission, denial response, payment posting, and follow-up. They don't just move paperwork. They keep reimbursement moving.
Demand for these roles reflects that reality. The employment of medical records specialists, which includes revenue cycle specialists, is projected to grow by 7 percent from 2024 to 2034, with about 14,200 openings each year on average according to the U.S. Bureau of Labor Statistics occupational outlook. That isn't just a labor trend. It's a signal that healthcare organizations increasingly depend on this function to maintain financial stability.
Table of Contents
- Introduction The Hidden Engine of Healthcare Profitability
- What Is a Revenue Cycle Specialist Really
- Core Responsibilities and Key Performance Indicators
- The Strategic Choice In-House Team vs Outsourced Partner
- How to Evaluate and Select the Right RCM Partner
- Common Pitfalls and How to Measure True ROI
- Conclusion Your Next Strategic Financial Move
Introduction The Hidden Engine of Healthcare Profitability
Healthcare leaders rarely need another definition of revenue cycle management. They need revenue they can collect, fewer preventable denials, and a billing operation that doesn't depend on heroic effort every month-end.
A revenue cycle specialist sits in the middle of that problem. This person works at the points where clinical activity becomes financial outcome. If patient access misses insurance details, if coding doesn't align cleanly with payer rules, or if denied claims sit too long without appeal, cash slows down. The specialist's job is to stop those failures before they become write-offs, patient complaints, or ugly A/R aging reports.
That's why the role deserves leadership attention. Revenue cycle specialists oversee payment and collections, track accounts receivable, support patient payment arrangements when needed, and keep reimbursement moving through hospitals and clinics. When they perform well, they strengthen both operational efficiency and financial predictability.
Leadership view: If your organization keeps talking about denials, lagging collections, or billing inconsistency, you don't have an abstract RCM problem. You have a process ownership problem.
The organizations that get the most value from revenue cycle specialists don't isolate them as task workers. They position them as financial operators with authority to identify trends, escalate payer issues, and tighten handoffs between front office, coding, billing, and finance.
That shift matters because reimbursement pressure won't ease on its own. Leaders need people who can translate payer complexity into disciplined workflow, compliant billing, and cleaner cash realization.
What Is a Revenue Cycle Specialist Really
Think of the revenue cycle as the organization's financial bloodstream. Care delivery creates the value. The revenue cycle carries that value from appointment to reimbursement. A revenue cycle specialist keeps that flow moving and clears the blockages when it doesn't.
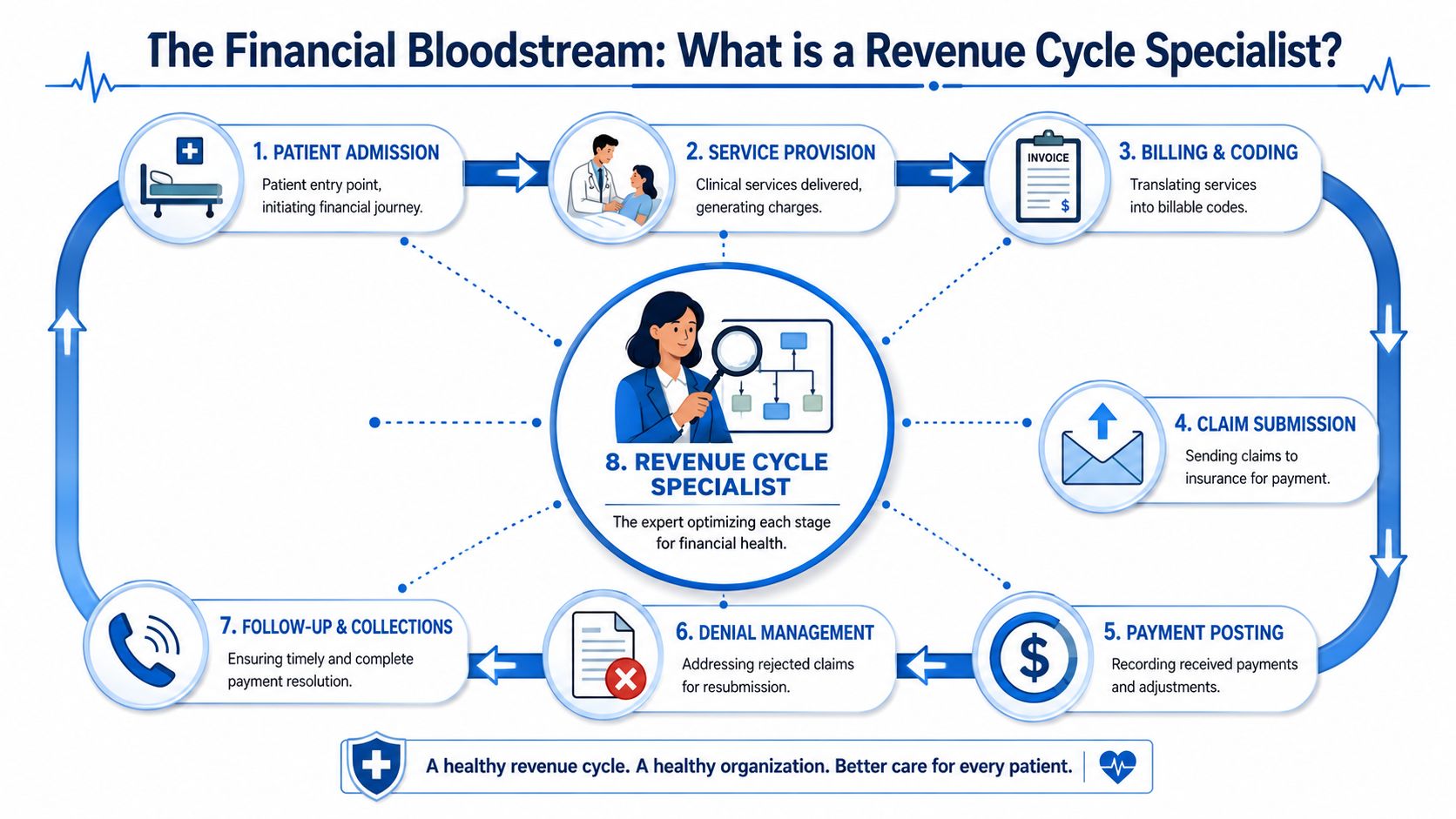
The role across the full financial journey
The role starts well before a claim is submitted. It begins when patient information is captured, insurance is verified, and financial responsibility is clarified. Weak execution at that stage creates downstream rework that no billing team can fully erase later.
From there, the specialist helps protect revenue through each major phase:
- Patient access and intake: They verify coverage, confirm demographic data, and reduce preventable registration errors.
- Charge capture and coding support: They help ensure clinical services are translated into billable data that aligns with payer requirements.
- Claims management: They submit claims, monitor rejections, and resolve edits before balances drift.
- Payment posting and variance review: They compare expected reimbursement to actual reimbursement and flag underpayments.
- Denial and A/R follow-up: They pursue corrections, appeals, and account resolution so receivables don't stall.
That full-cycle view is what separates revenue cycle specialists from narrower billing roles. In many organizations, they function much like a medical claims analyst, but with broader accountability across operational and financial touchpoints.
Why leadership should treat the role strategically
The role also requires technical depth. Effective revenue cycle specialists need detailed knowledge of Medicare and managed care reimbursement methodologies, coding standards such as ICD-10, CPT, and HCPC, and billing forms including CMS 1500 and UB-04, as described by this overview of certified revenue cycle specialist competencies. That isn't clerical knowledge. It's specialized reimbursement expertise.
A mature specialist does more than process work. They identify denial patterns, spot payment variances, and recognize where policy, workflow, or training failures are draining revenue. They also understand the compliance boundary. Billing speed without coding accuracy or HIPAA discipline only moves risk faster.
A good revenue cycle specialist doesn't ask, “Was the claim sent?” They ask, “Was the claim built correctly, paid correctly, and followed to final resolution?”
For executives, that distinction changes the hiring conversation. You're not filling a seat. You're assigning ownership over one of the most vulnerable financial systems in the organization.
Core Responsibilities and Key Performance Indicators
The easiest way to misunderstand revenue cycle specialists is to list tasks without connecting them to financial results. Leadership doesn't need a job description. Leadership needs to know which actions improve cash performance, reduce leakage, and surface risk early.

Front-end control points
Front-end work is where many costly failures begin. Eligibility errors, incomplete authorization workflows, and inaccurate patient data create claims that look finished but aren't payable.
Revenue cycle specialists typically own or influence several high-impact controls:
- Insurance verification: Coverage and benefit validation reduce avoidable claim rejections.
- Registration accuracy: Clean demographic and subscriber data support cleaner claim submission.
- Financial responsibility communication: Patients are less likely to be surprised when estimates and billing pathways are discussed early.
- Documentation and coding coordination: Strong handoffs reduce coding mismatches and payer edits.
The KPI connection is direct. Better front-end discipline usually improves clean claim performance, lowers initial rejections, and reduces back-end rework. Executives often track these through denial trends, first-pass claim acceptance, and collection efficiency indicators.
A specialist operating at a high level doesn't just correct errors. They identify where the process keeps producing the same error and push the fix upstream.
Back-end recovery and cash acceleration
Once claims move out the door, the work shifts from prevention to realization. At this stage, many organizations leave money uncollected because follow-up is inconsistent, underpayments aren't challenged, or denials don't receive structured appeal.
Revenue cycle specialists manage that pressure through:
- Payment posting oversight that reveals whether actual reimbursement matches payer expectations.
- Variance analysis to identify underpayments and reimbursement irregularities.
- Denial management with root-cause review, correction, and appeal.
- Accounts receivable follow-up to prevent balances from aging unnecessarily.
- Patient payment support when balances require clarification or structured arrangements.
For leaders tracking cash, these tasks affect A/R aging, collection velocity, and overall net recovery. If you want a practical benchmark for one of the central measures, this explanation of net collection rate is the right place to start because it ties daily revenue cycle discipline to collectible revenue.
Here is a helpful perspective:
| Operational activity | What the specialist is watching | What leadership should watch |
|---|---|---|
| Eligibility and registration | Missing data and coverage issues | Front-end error patterns |
| Claim submission | Edits, rejections, payer formatting issues | Clean claim consistency |
| Payment posting | Underpayments and unusual adjustments | Reimbursement integrity |
| Denial work | Root causes and appeal status | Denial trend movement |
| A/R follow-up | Timeliness and unresolved balances | Aging and cash conversion |
A closer look at workflow helps. The short video below offers a useful visual primer on how these handoffs affect reimbursement.
Operational warning: If your team reviews denials only after month-end reporting, you're measuring damage after it has already hit cash.
The strongest specialists don't work passively from assigned queues. They manage a living control system that connects payer rules, coding discipline, account follow-up, and reporting back to financial leadership.
The Strategic Choice In-House Team vs Outsourced Partner
At some point, leadership has to make a structural decision. Should the organization build its own revenue cycle specialist team, or should it partner with an outside firm that provides the function at scale?
That decision shouldn't be driven by instinct. It should be based on cost structure, available expertise, management capacity, and how much operational variability your organization can tolerate.
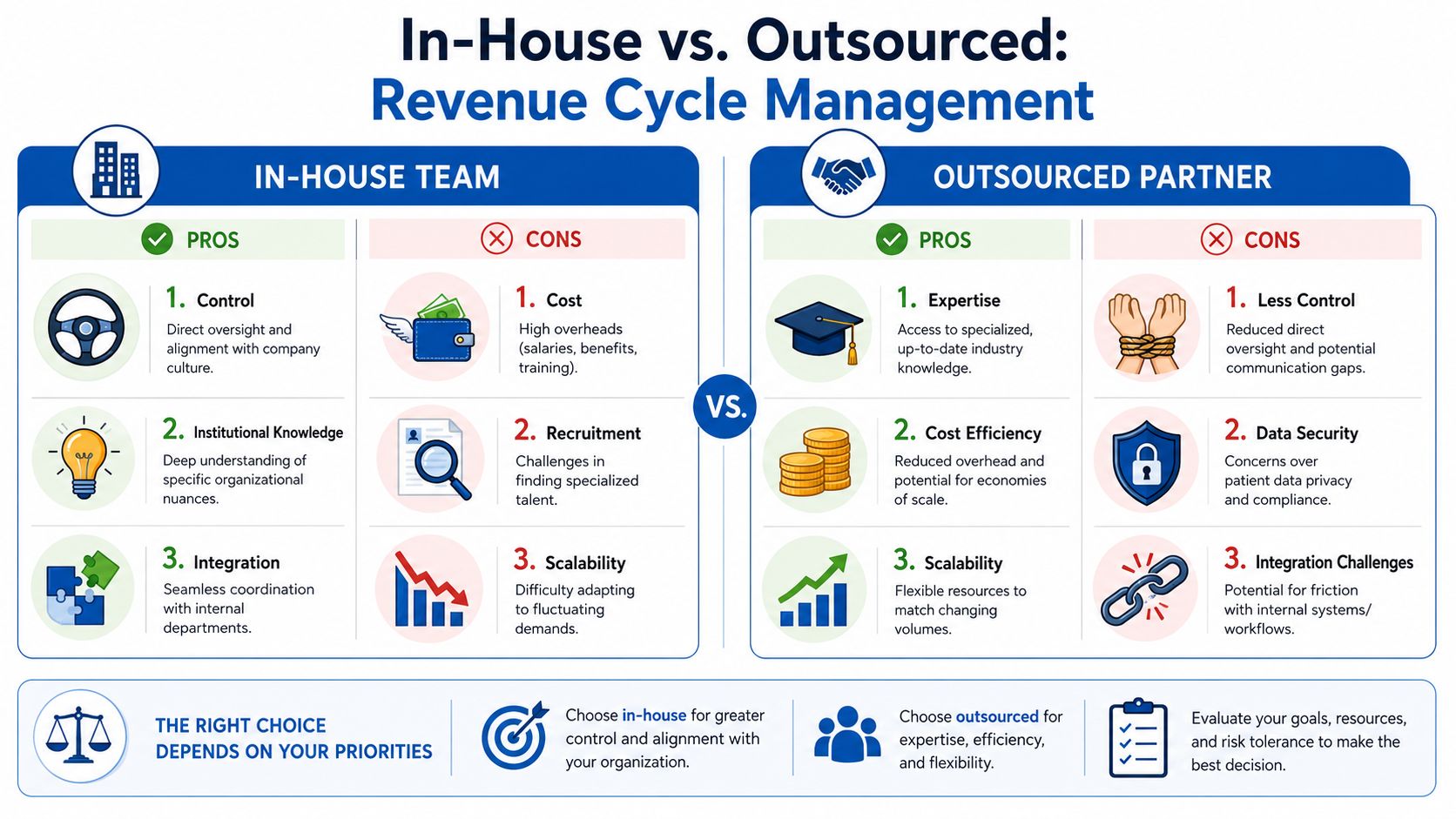
What in-house really buys you
In-house teams give leaders direct oversight. They usually integrate more naturally with scheduling, front desk workflows, clinic managers, and internal finance. That matters when the organization needs fast cross-functional decisions or highly customized processes.
But control has a cost. As of July 2026, the average annual salary for a Revenue Cycle Specialist is $68,202, with a typical range of $55,816 to $73,538, according to Salary.com's Revenue Cycle Specialist salary data. That's only the direct compensation layer. Internal teams also require onboarding, supervision, workflow design, technology alignment, coverage planning, and continuous training as payer requirements change.
An in-house model tends to work best when leadership already has strong RCM management infrastructure and enough scale to support specialization without creating single points of failure.
What outsourcing changes
An outsourced model changes the economics and the operating model. Instead of building all expertise internally, the organization buys access to specialists, management process, and often a more structured reporting cadence.
That can help when internal staffing is thin, denial work has become inconsistent, or leadership wants faster implementation without a long recruiting cycle. It also gives organizations a way to scale support up or down as volumes and priorities shift.
The trade-off is that outsourcing only works when the partner integrates well with clinical operations and communicates clearly. If the vendor operates as a detached billing factory, denials may still move, but patient confusion and internal friction will rise.
One example of this outsourced model is medical billing services from Clarity Health RCM, which can support organizations that want either end-to-end management or targeted help in selected billing functions.
In-House vs. Outsourced RCM A Comparison
| Factor | In-House Specialists | Outsourced Partner (e.g., Clarity Health RCM) |
|---|---|---|
| Control | Direct day-to-day oversight | Requires governance and communication structure |
| Institutional knowledge | Deep familiarity with local workflows | Must be built through onboarding and collaboration |
| Staffing risk | Vacancies and turnover can disrupt collections | Broader bench can reduce dependence on one person |
| Cost model | Salary plus management and operating overhead | Usually structured as an external service investment |
| Scalability | Harder to expand quickly | Easier to adjust support to workload |
| Technology discipline | Depends on internal capability | Often comes with established process and reporting cadence |
| Patient financial experience | Easier to keep close to the care team | Must be intentionally integrated to avoid disconnect |
The wrong comparison is “employee versus vendor.” The right comparison is “fixed overhead versus managed capability.”
The best choice depends on organizational maturity. If your internal operation is disciplined and well-led, in-house can work well. If your denials are climbing, your reporting is inconsistent, or key billing knowledge lives in too few people, outsourcing can be the safer financial decision.
How to Evaluate and Select the Right RCM Partner
Most RCM partnerships look similar in a sales presentation. They talk about technology, expertise, follow-up, and reporting. The difference shows up after implementation, when your staff starts asking who owns unresolved accounts, who handles patient confusion, and who is accountable when payer edits keep recurring.
A useful evaluation process starts with operational specificity. Ask the partner to walk through exactly how they manage intake handoffs, claim edits, denial routing, payment variance review, patient calls, and escalation to your leadership team. General assurances aren't enough. You need workflow answers.
Questions leadership should press on
Use diligence questions that expose process maturity:
- Reporting discipline: What do they report routinely on denial trends, underpayments, A/R work queues, and unresolved payer issues?
- Specialty and payer fit: Can they explain how they handle your major payer mix and specialty-specific billing challenges?
- Escalation model: When a denial pattern appears, who investigates root cause and who owns corrective action?
- Compliance depth: How do they protect HIPAA requirements and maintain documentation discipline across teams?
- Operational integration: How do they work with front desk, coding, clinical leadership, and finance rather than around them?
A good partner should answer those questions plainly. If they can't explain their operating model in detail, they probably can't run it consistently.
Ask for reporting samples before contract signature. If the data isn't clear in the sales process, it won't get clearer after go-live.
The patient experience test
This is the area leaders often miss. Outsourcing may improve workflow, but if it weakens the patient's financial experience, the organization pays for it elsewhere through confusion, complaints, and trust erosion.
That risk is real. Undue Medical Debt's perspective on navigating healthcare finances notes that patients can feel disconnected from billing staff when revenue cycle work is outsourced, and that disconnect can create confusion and erode trust. The practical implication is simple. Don't select a partner until you understand how they preserve a person-centered support model.
Look for signs of maturity here:
- Named ownership: Patients and staff should know who handles questions and escalations.
- Warm handoffs: On-site and remote teams should share clear procedures for transferring billing issues without forcing patients to restart the story.
- Financial empathy: Scripts and workflows should help patients understand balances, coverage, and assistance pathways in plain language.
- Shared accountability: Patient experience shouldn't sit outside revenue cycle reporting.
A partner can be technically capable and still be a poor fit if they create distance between billing and care. In healthcare, financial operations aren't separate from the patient relationship. They're part of it.
Common Pitfalls and How to Measure True ROI
Organizations often miss the value of revenue cycle specialists because they measure the wrong things. They compare staffing cost to contract cost and stop there. That's incomplete.
ROI in revenue cycle work shows up in revenue protection, faster resolution, cleaner payer execution, and fewer avoidable handoffs between departments. If you only ask whether the function costs less, you ignore whether it performs better.
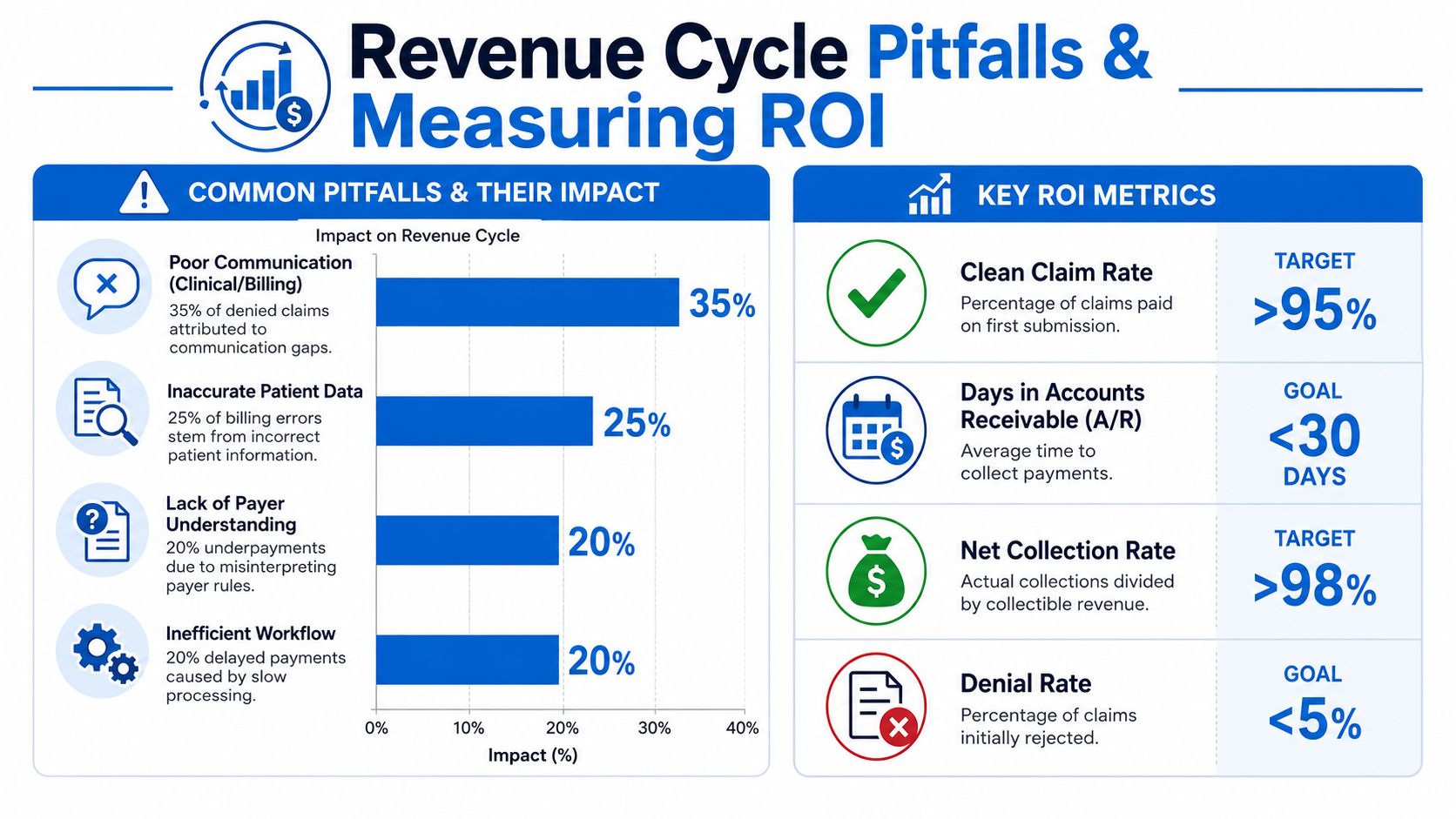
Where organizations misjudge value
The most common mistake is choosing a model based on apparent savings while tolerating weak execution. Cheap denial management isn't cheap if underpayments go unchallenged. A low vendor fee isn't a win if patient billing confusion increases and staff spend more time cleaning up miscommunication.
Another mistake is poor implementation. Even a capable internal hire or outsourced partner will struggle if your organization doesn't define ownership, escalation pathways, and reporting cadence early. Revenue cycle specialists need authority and visibility. Without both, they become task handlers instead of problem-solvers.
How to frame ROI for the C-suite
A stronger approach is to evaluate performance through management indicators that connect directly to cash and organizational stability. High-performing revenue cycle specialists are measured by exceeding Net Promoter Score goals, tracking denial trends to ensure full reimbursement, and maintaining aggressive follow-ups on accounts receivable to reduce aging, as outlined by The Chappelle Group's description of specialist benchmarks.
For executive review, focus on questions like these:
- Are denial patterns shrinking because root causes are being fixed, not just worked?
- Is receivable aging improving because follow-up is disciplined and timely?
- Are underpayments being identified and challenged rather than merely posted?
- Does patient financial communication improve or deteriorate after operational changes?
- Is reporting giving leadership earlier visibility into reimbursement risk?
A revenue cycle function earns its keep when leadership can see fewer surprises, faster resolution, and clearer control over collectible revenue.
That's the essential ROI frame. Better revenue cycle performance doesn't just support finance. It supports planning. A hospital can make stronger staffing, growth, and capital decisions when reimbursement is managed with consistency instead of hope.
Conclusion Your Next Strategic Financial Move
Revenue cycle specialists sit closer to financial performance than many leadership teams realize. They influence whether services turn into cash cleanly, whether denials become recoverable or permanent, and whether patient billing feels navigable or adversarial.
That makes this role strategic. Not because the title sounds senior, but because the work affects profitability, risk exposure, patient trust, and the reliability of your reporting. Whether you build internally or outsource, the standard should be the same: clear accountability, strong payer knowledge, disciplined follow-up, useful reporting, and tight integration with your care teams.
If your organization is still treating revenue cycle work as administrative cleanup, you're likely leaving value on the table. The better approach is to treat revenue cycle specialists as part of the financial operating core of the enterprise. That's how organizations improve collections without losing compliance discipline or damaging the patient experience.
Leadership doesn't need more activity in the revenue cycle. It needs better control.
A practical next step is to get an outside view of where your current process is breaking down. Clarity offers a complimentary consultation of your revenue cycle and can outline either full-service support or targeted help for specific billing gaps.
No responses yet