A lot of hospital leaders land on the same question after a rough month close. Cash came in lighter than expected, case mix looks off, and someone from compliance is suddenly worried about a payer request for records. On paper, coding was completed and claims went out. In practice, the inpatient story may not have been translated accurately into the final DRG.
That's why so many finance and clinical leaders end up asking what is DRG validation, and why it matters beyond billing. A weak validation process doesn't just create underpayments or repayment risk. It can also distort how your organization is represented in quality reporting, especially when diagnosis selection and Present on Admission reporting are wrong.
Table of Contents
- Why Inaccurate DRGs Are a Hidden Drain on Your Hospital
- What Is DRG Validation Really
- The DRG Validation Process and Key Stakeholders
- Common DRG Errors and Payer Audit Triggers
- The Financial and Quality Impact of DRG Validation
- Building Your DRG Validation Strategy
- How Clarity Elevates Your Revenue Cycle
Why Inaccurate DRGs Are a Hidden Drain on Your Hospital
The usual version of this problem starts subtly. Finance sees inpatient reimbursement trending below expectations. HIM says coding turnaround is on track. CDI reports strong query volume. Then a payer audit exposes something more fundamental. The chart supports one clinical story, but the billed DRG reflects another.
A Diagnosis-Related Group, or DRG, is the payment framework that translates an inpatient stay into a reimbursement category. If the principal diagnosis is wrong, if a procedure isn't supported, or if a Present on Admission indicator is inaccurate, the payment outcome changes. So does your compliance exposure.
What makes this expensive is that the damage rarely stays inside one claim. The same documentation habits, sequencing mistakes, and communication gaps tend to repeat across service lines. That's why a hospital that only treats DRG issues as billing cleanup usually stays reactive.
For finance leaders, the bigger issue is control. You need a way to confirm that the final billed DRG matches the actual clinical record before or soon after the claim leaves the building. That's the work of DRG validation. It sits between coding, clinical documentation, compliance, and payment integrity.
Practical rule: If your team only reviews DRG accuracy after denials or audits arrive, you're paying to discover problems late.
A strong validation program also supports adjacent revenue work. Many organizations first notice DRG weakness when they start examining broader medical revenue recovery opportunities and realize the same root cause keeps surfacing: the record wasn't translated into a defensible claim.
Why this doesn't behave like a simple billing issue
A coding error can be isolated. A DRG validation failure usually isn't. It often signals one or more of these breakdowns:
- Clinical ambiguity: The physician documented a condition loosely, and the chart never clearly established severity, cause, or timing.
- Sequencing weakness: Coders had valid codes available, but the principal diagnosis selected didn't align with the reason for admission after study.
- Documentation mismatch: Progress notes, labs, orders, and discharge summary told slightly different stories.
- Operational silos: CDI, coders, and finance all saw parts of the problem, but nobody owned the final defense of the DRG.
That's why inaccurate DRGs are such a hidden drain. They reduce payment accuracy, increase audit risk, and blur the quality picture leadership depends on.
What Is DRG Validation Really
At a surface level, DRG validation sounds like a coding check. It's more than that. DRG validation is a structured review of whether the assigned DRG is clinically supported, coded correctly, and defensible under payer scrutiny.
A useful analogy is editorial review. Routine coding is like writing the chapter summary. DRG validation is the editor checking the summary against the entire book. The reviewer asks whether the principal diagnosis, secondary diagnoses, procedures, and POA logic match the full patient story.
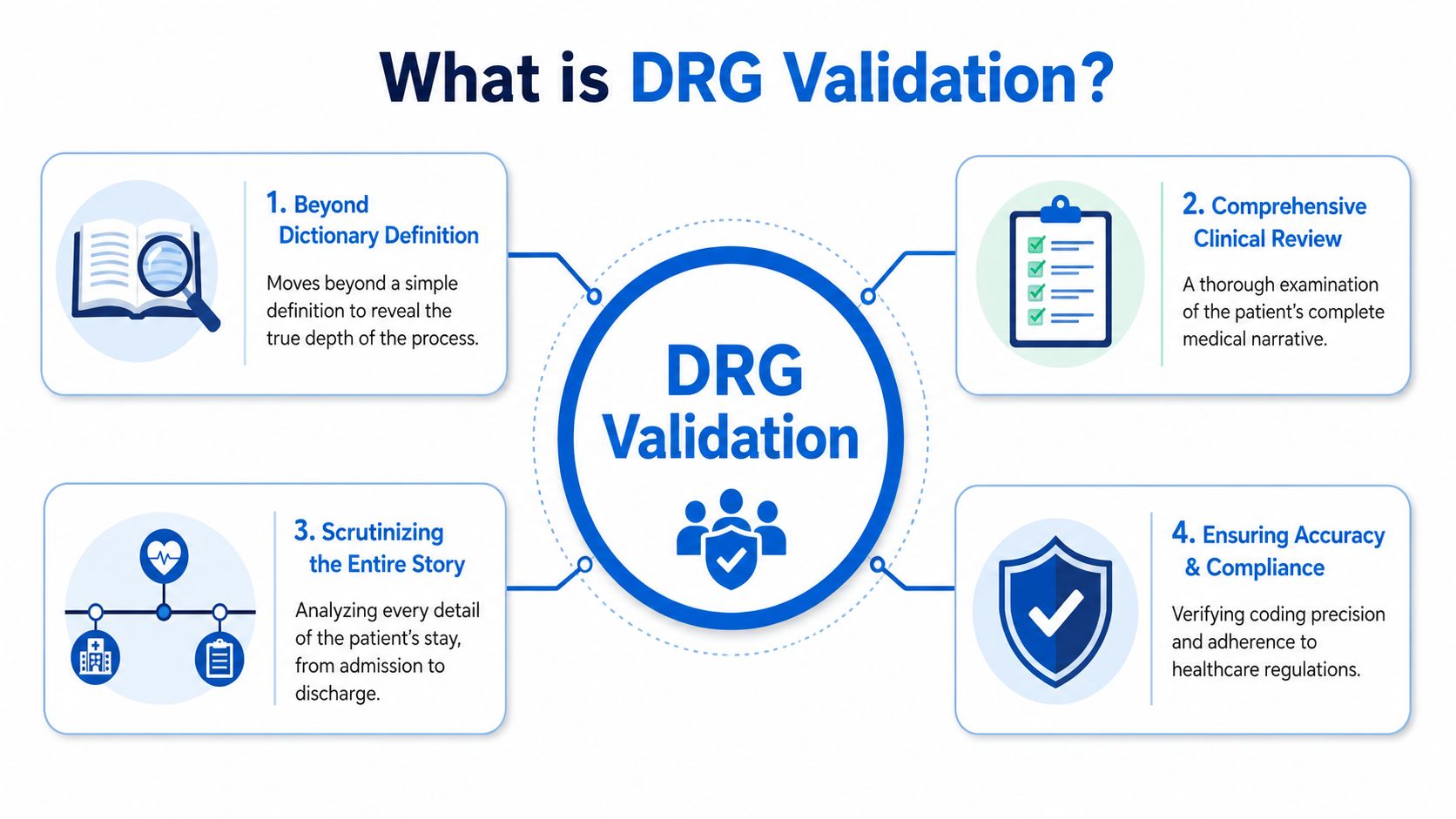
It tests the whole clinical narrative
When people ask what is DRG validation, the best answer is this: it confirms that the final inpatient payment category reflects the care that was delivered.
That means a reviewer looks beyond code assignment and asks harder questions:
- Was the principal diagnosis really the condition chiefly responsible for the admission?
- Do the secondary diagnoses have clear physician support and clinical evidence in the chart?
- Were the procedures captured in a way that matches the operative note and the coding rules?
- Do the POA indicators align with the record timeline?
Many organizations encounter difficulties in this area. A coded claim can be technically complete and still fail validation because the record doesn't support the severity implied by the DRG.
What validation confirms before a claim stands up
A good validator doesn't just look for missed revenue. They also look for unsupported revenue. Both matter.
Here's what a solid review usually confirms:
Clinical consistency
The attending note, consultant documentation, orders, imaging, labs, and discharge summary should support one coherent story.Coding defensibility
The ICD-10-CM and ICD-10-PCS choices should be accurate, but accuracy alone isn't enough if sequencing logic is weak.Payment integrity
The assigned DRG should reflect the patient's acuity and the resources consumed, not merely the highest-paying plausible option.
A defensible DRG is one you can explain from the chart without adding assumptions after the fact.
The distinction matters for CFOs because validation is one of the few processes that directly connects clinical documentation to financial reliability. It tells leadership whether the hospital is billing what happened, not what the team hoped the chart meant.
The DRG Validation Process and Key Stakeholders
The process works best when it's operationally clear. Hospitals that struggle with DRG validation usually don't fail because staff lack effort. They fail because no one has defined where review happens, which cases get priority, and who resolves disagreements.
How the workflow actually runs
Most programs use some mix of pre-bill and post-bill review. Pre-bill validation is better for prevention. Post-bill validation is useful for trend analysis, education, and identifying systemic exposure.
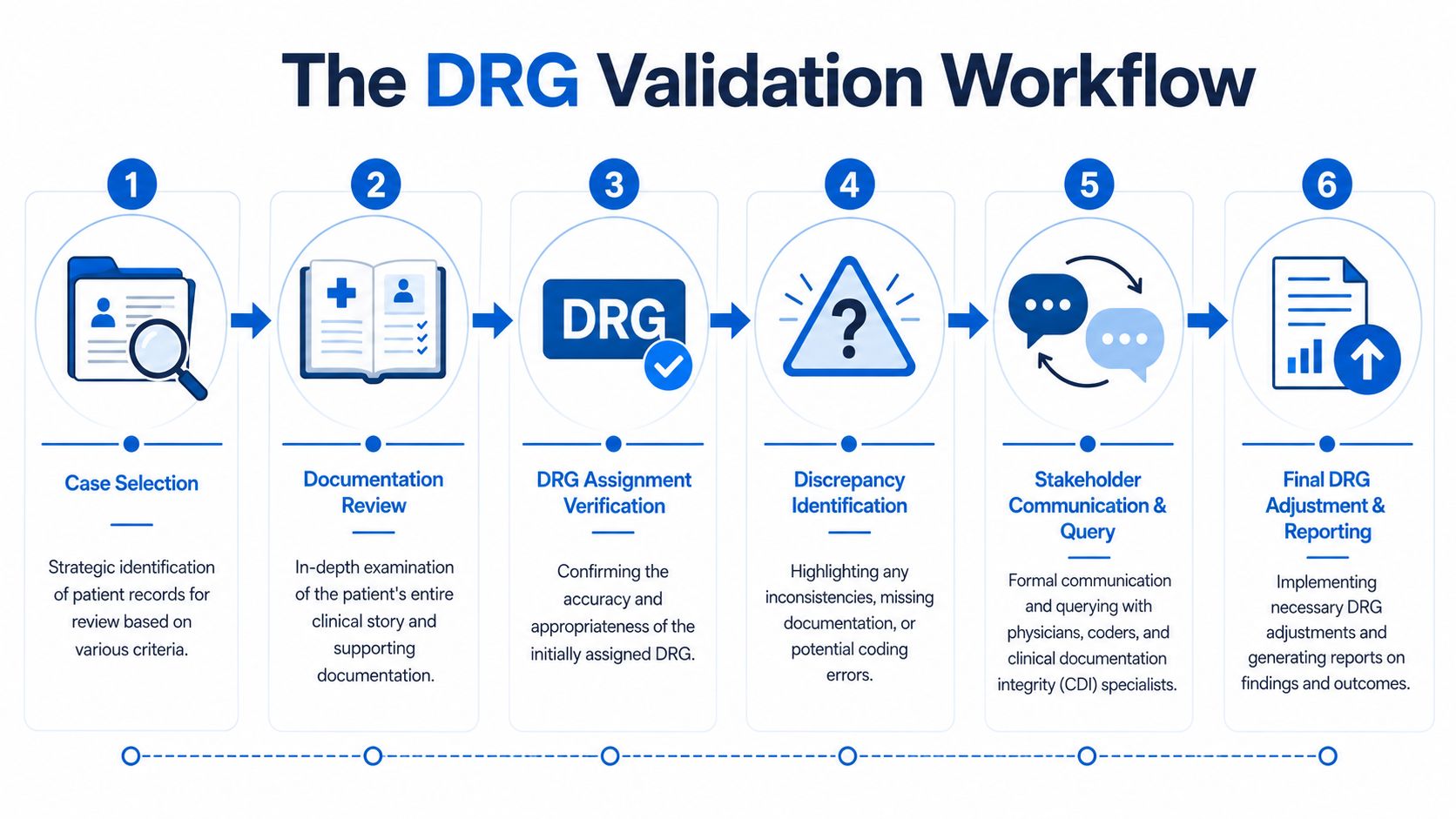
The workflow usually looks like this:
Case selection
Teams target records based on risk. That may include high-acuity service lines, short stays, frequent denials, unusual DRG patterns, or diagnoses with known documentation sensitivity.Full chart review
A qualified auditor reviews the medical record as a clinical and coding narrative, not just a code set. Such a review reveals unsupported severity, weak principal diagnosis selection, and POA concerns.DRG verification
The reviewer checks whether the billed DRG is supported or whether a different grouping is more accurate and defensible.Discrepancy escalation
If a concern is found, the issue goes back to coding, CDI, or physician leadership depending on the problem.Correction and reporting
The claim is adjusted if appropriate, and leadership gets trend reports that show recurring failure points.
Hospitals that want a sharper view of this handoff often benefit from understanding the role of a medical claims analyst because many of the practical review skills overlap. Pattern recognition, documentation review, variance analysis, and clear escalation matter here too.
Who owns each part of the outcome
DRG validation is cross-functional by design. That's why weak governance causes so much friction.
| Stakeholder | Primary role in DRG validation | What goes wrong without them |
|---|---|---|
| CDI specialists | Clarify clinical specificity and identify documentation gaps | Severity is implied but not explicitly supported |
| Coders | Apply code selection and sequencing rules correctly | The coded claim may be complete but not defensible |
| Physicians | Document the patient's condition, treatment, and causality clearly | The record becomes vulnerable to clinical validation challenges |
| Auditors | Test the chart against coding and clinical logic | Errors remain hidden until a payer finds them |
| Finance and RCM leaders | Set priorities, monitor trends, and fund the process | Validation becomes sporadic and reactive |
The strongest programs don't treat DRG validation as an HIM task. They treat it as a shared control over inpatient revenue integrity.
What works is a defined escalation path. What doesn't work is sending audit findings into email chains where coding, CDI, and physician leadership each wait for the other side to move first.
Common DRG Errors and Payer Audit Triggers
Payers rarely need a dramatic failure to challenge a DRG. They look for predictable weaknesses. If your documentation and coding practices produce the same questionable patterns repeatedly, you've created your own audit target.
Where teams get into trouble
The most common DRG errors tend to fall into a few categories.
Principal diagnosis errors happen when the condition selected as the reason for admission doesn't align with the actual clinical course. A classic example is when the chart supports one condition as the true driver of admission, but a less appropriate diagnosis gets sequenced first.
CC and MCC capture failures show up in two directions. Sometimes the hospital misses supported complications or comorbidities and loses legitimate payment. Other times the record contains a coded CC or MCC that the chart doesn't really support, which is exactly the kind of issue payers attack.
Procedure support problems occur when the coded procedure doesn't match the operative detail or when the procedure was captured in a way that changes grouping without solid documentation behind it.
POA mistakes are especially dangerous because they affect more than reimbursement. When a condition's timing is wrong, the hospital may misstate whether it was present at admission or acquired during the stay.
Here's a practical view of the issues teams see most often:
| Error Type | Example | Financial/Compliance Impact |
|---|---|---|
| Incorrect principal diagnosis | The chart supports one admission-driving condition, but another diagnosis is sequenced as principal | Wrong DRG assignment, underpayment or overpayment risk, appeal difficulty |
| Missed CC or MCC | A clinically supported secondary condition isn't captured clearly enough to code | Lost reimbursement and weaker severity representation |
| Unsupported CC or MCC | A high-severity secondary diagnosis is coded, but the chart evidence is thin | Payer downgrade, recoupment, clinical validation denial |
| Unsupported procedure coding | The procedure code changes grouping, but documentation is incomplete or inconsistent | Audit exposure and rebill work |
| Incorrect POA indicator | A condition developing after admission is flagged as present on admission, or the reverse | Quality reporting distortion and compliance risk |
For a wider operational view of how these mistakes spread through revenue cycle workflows, it helps to review common medical coding errors and where controls usually break down.
Patterns that attract payer attention
Payers don't need to audit every chart. They look for patterns that suggest weak internal controls.
Common triggers include:
- High use of a narrow set of high-severity diagnoses
- Repeated downgrades in the same service line
- Short inpatient stays with complex DRG assignments
- Frequent disagreement between clinical documentation and coded severity
- POA patterns that look inconsistent with the underlying record
A single bad case is painful. A recognizable pattern is what brings sustained scrutiny.
The Financial and Quality Impact of DRG Validation
Most leaders first approve DRG validation because they want cleaner reimbursement. That's reasonable, but it's only half the business case.
Revenue protection is only half the case
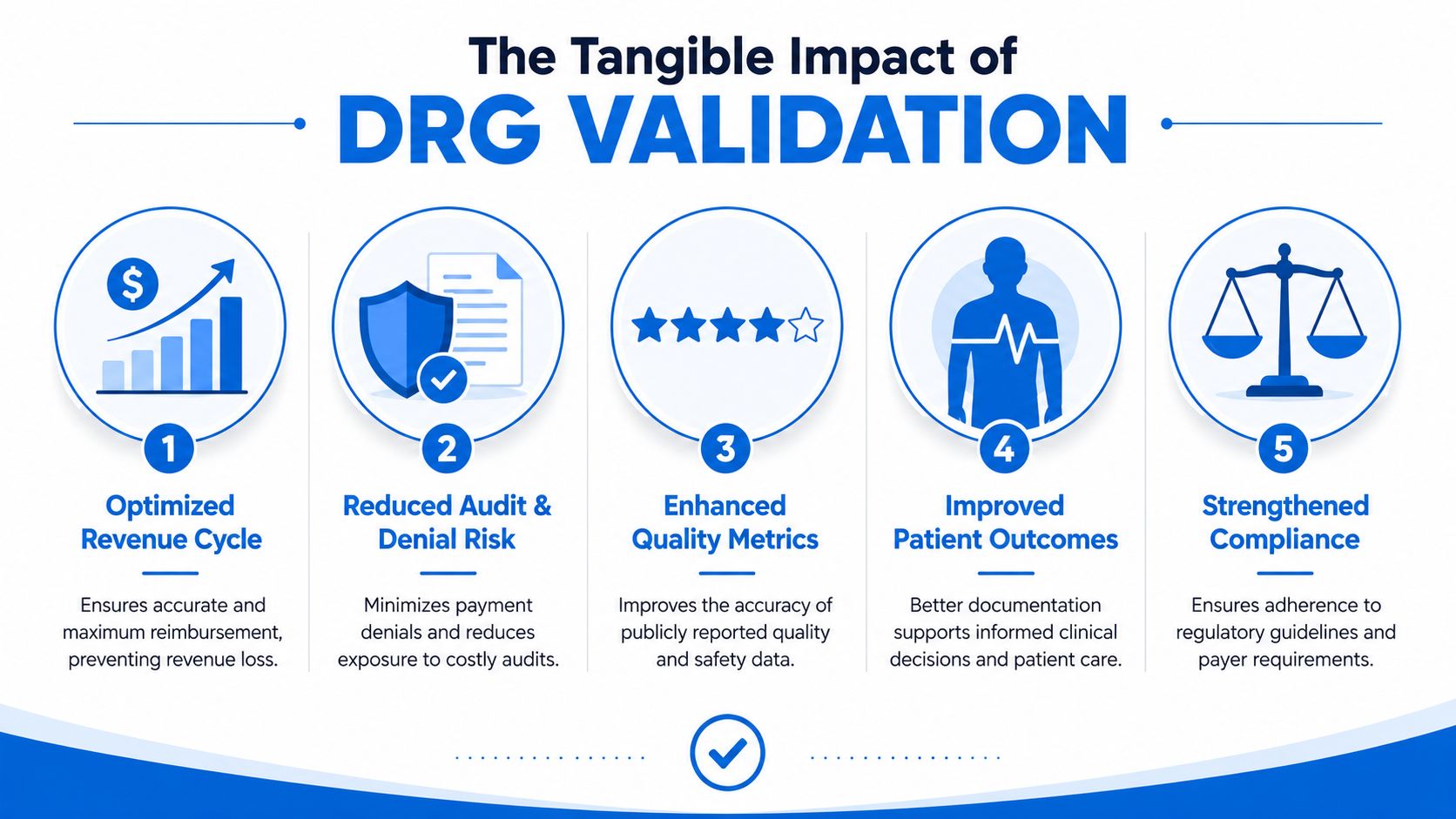
At the financial level, DRG validation protects both sides of the ledger. It helps the hospital avoid underbilling when severity is missed, and it helps prevent repayment risk when severity is overstated or unsupported.
That matters because inpatient margin problems often begin with small documentation and sequencing failures that repeat across many cases. Finance sees the effect as payment variance, denials, late appeals, and unstable forecasting. Operations feel it as coder rework, CDI backlog, and more chart defense after the bill has already gone out.
A mature validation process changes the timing of that pain. Instead of discovering weaknesses when a payer asks for records, the hospital identifies them when correction is still practical.
This short explainer captures why hospitals increasingly connect DRG review to broader performance:
Why quality leaders should care as much as finance
This is the part most articles miss. DRG validation also protects your quality metrics and public credibility.
According to the AAPC discussion of DRG coding validations, 34% of DRG validation audits in the last 12 months revealed that principal diagnosis miscoding, not just secondary coding errors, caused incorrect HAC/POA flagging, which CMS uses to penalize hospitals in quality reporting. That's the clearest argument for treating DRG validation as more than a revenue recovery function.
If the principal diagnosis is wrong, or if POA logic is wrong, a hospital can report the wrong story about whether a complication was hospital-acquired or present before admission. Payment may still be affected, but so are the metrics that clinical leaders, boards, and regulators care about.
When DRG validation fails, the hospital doesn't just risk the wrong payment. It risks the wrong quality profile.
That changes the audience for this work. DRG validation belongs to the CFO, but it also belongs to quality leadership, physician advisors, compliance, and case management. It protects reimbursement, yes. It also protects how your hospital is measured.
Building Your DRG Validation Strategy
Hospitals get better results when they treat DRG validation as an operating model decision, not a side project. The first choice isn't software. It's ownership.

Choose the operating model first
Some organizations build an internal validation team. That can work well if you have stable inpatient coding leadership, strong CDI coverage, physician advisor support, and reliable reporting infrastructure.
Others use an external partner for all or part of the function. That approach often works better when staffing is thin, denial pressure is rising, or leadership wants an outside read on entrenched documentation habits.
The trade-offs are straightforward:
- In-house model: Better day-to-day visibility, but harder to staff and harder to keep fully objective.
- External model: Faster access to specialized review talent, but only valuable if the partner can integrate with your workflow and communicate findings clearly.
- Hybrid model: Often the most practical. Internal teams manage concurrent work and physician engagement. External reviewers handle focused audits, trend analysis, or overflow.
Questions leadership should ask now
If you're assessing your current state, start with the questions that reveal process maturity:
Where do DRG issues surface today
Before billing, after denial, during appeal, or only during payer audit?Which teams can challenge a weak principal diagnosis
If no one can escalate that issue confidently, the process is not mature.How clear is the CDI to coder handoff
Ambiguity here usually shows up later as inconsistent severity capture.Do physicians receive focused feedback
Generic education rarely changes documentation behavior.Can finance see trend-level findings
Leadership needs more than case anecdotes. They need categories, recurrence, and operational causes.
A practical strategy usually includes these actions:
- Define review scope: Decide which cases get pre-bill review and which are sampled post-bill.
- Set escalation rules: Spell out who resolves coding disputes, clinical support concerns, and POA conflicts.
- Standardize reporting: Give finance, HIM, CDI, and quality a shared view of findings.
- Close the loop: Use validation outcomes for education, not just claim correction.
What works is consistency. What doesn't work is launching a one-time audit, finding problems, and assuming awareness alone will fix them.
How Clarity Elevates Your Revenue Cycle
If you've read this far, the core point is simple. DRG validation is not a narrow coding exercise. It's a control point that connects inpatient documentation, reimbursement accuracy, audit defense, and quality reporting.
For CFOs, that means stronger revenue integrity and fewer unpleasant surprises after payment. For clinical and quality leaders, it means greater confidence that coded data reflects the actual patient story, including the accuracy of HAC and POA reporting. For operations, it means less rework and a clearer path from chart to clean claim.
Building that capability internally takes time, staffing, and discipline. Many organizations need help creating the workflow, reporting structure, and review rigor that make validation useful instead of theoretical. That's where an experienced RCM partner can add value, especially when support has to extend beyond one audit cycle and into the daily mechanics of billing operations, payment posting, insurance follow-up, and front-end process design.
If you want a practical review of where your revenue cycle is leaking value, Clarity offers a complimentary consultation focused on operational gaps, billing performance, and opportunities to strengthen financial outcomes without pulling your team away from patient care.
No responses yet