A familiar conversation is happening in medical groups right now. The CFO sees steady visit volume, the physicians are working, claims are going out, and yet cash still feels tight. Denials keep resurfacing. Aged receivables don't move fast enough. The billing team says claims were submitted. Leadership still asks the same question: if billing is happening, why isn't revenue landing the way it should?
That's usually the wrong framing. The actual issue isn't whether claims are being sent. It's whether the practice has built a system that prevents preventable revenue loss before a claim ever exists.
That's the difference in medical billing vs Revenue Cycle Management. One is a necessary function. The other is the operating model that determines whether that function can work consistently. If your organization is deciding whether to keep a billing-only setup, expand into full RCM, or outsource part of the process, the decision affects cash flow, staff workload, denial pressure, and financial visibility.
Table of Contents
- Is Your Billing Process Leaking Revenue
- Medical Billing Is a Task Revenue Cycle Management Is a System
- Comparing Medical Billing and RCM Across Key Functions
- Quantifying the ROI of Adopting Full Revenue Cycle Management
- Deciding Between In-House and Outsourced Financial Operations
- A Checklist for Choosing Your Financial Management Model
- How Clarity Health RCM Delivers Comprehensive Financial Care
Is Your Billing Process Leaking Revenue
A practice manager opens the month-end report and sees the same pattern again. Charges were entered. Claims were filed. Staff worked denials. Patient statements went out. But collections still lag expectations, and nobody can point to a single operational fix that will stop the problem from repeating next month.
That's the moment when leadership needs to separate a billing problem from a revenue cycle problem.
If the issue is purely tactical, a billing team can often correct it. Maybe payment posting is behind. Maybe follow-up work queues aren't being touched consistently. Maybe statements are going out late. Those are execution failures, and they matter.
But many organizations discover the revenue loss started earlier. The wrong subscriber ID entered at registration. An authorization that never got confirmed. A coverage change missed before the date of service. A charge capture handoff that left a service undocumented. By the time billing sees the claim, the damage is already built into it.
Practical rule: If your team spends most of its energy fixing denials after submission, you're probably dealing with a broken cycle, not just an overworked billing office.
Leadership should also pay attention to where financial conversations happen inside the practice. If revenue discussions begin only after claims age, the organization is operating too late in the process. Mature finance operations monitor front-end accuracy, coding integrity, payer behavior, denial patterns, and collection efficiency together.
That's why metrics such as net collection rate matter. They don't just show what was collected. They show whether the organization is consistently turning earned revenue into cash or losing part of it through preventable friction.
The practical takeaway is simple. Don't ask only, “Is billing being done?” Ask, “Where in the patient financial journey are we losing control?” That question usually leads to a better answer, and a different operating model.
Medical Billing Is a Task Revenue Cycle Management Is a System
Medical billing and Revenue Cycle Management work together, but they aren't interchangeable. Treating them as if they are usually leads to underinvestment in the parts of the process that decide whether reimbursement happens smoothly.
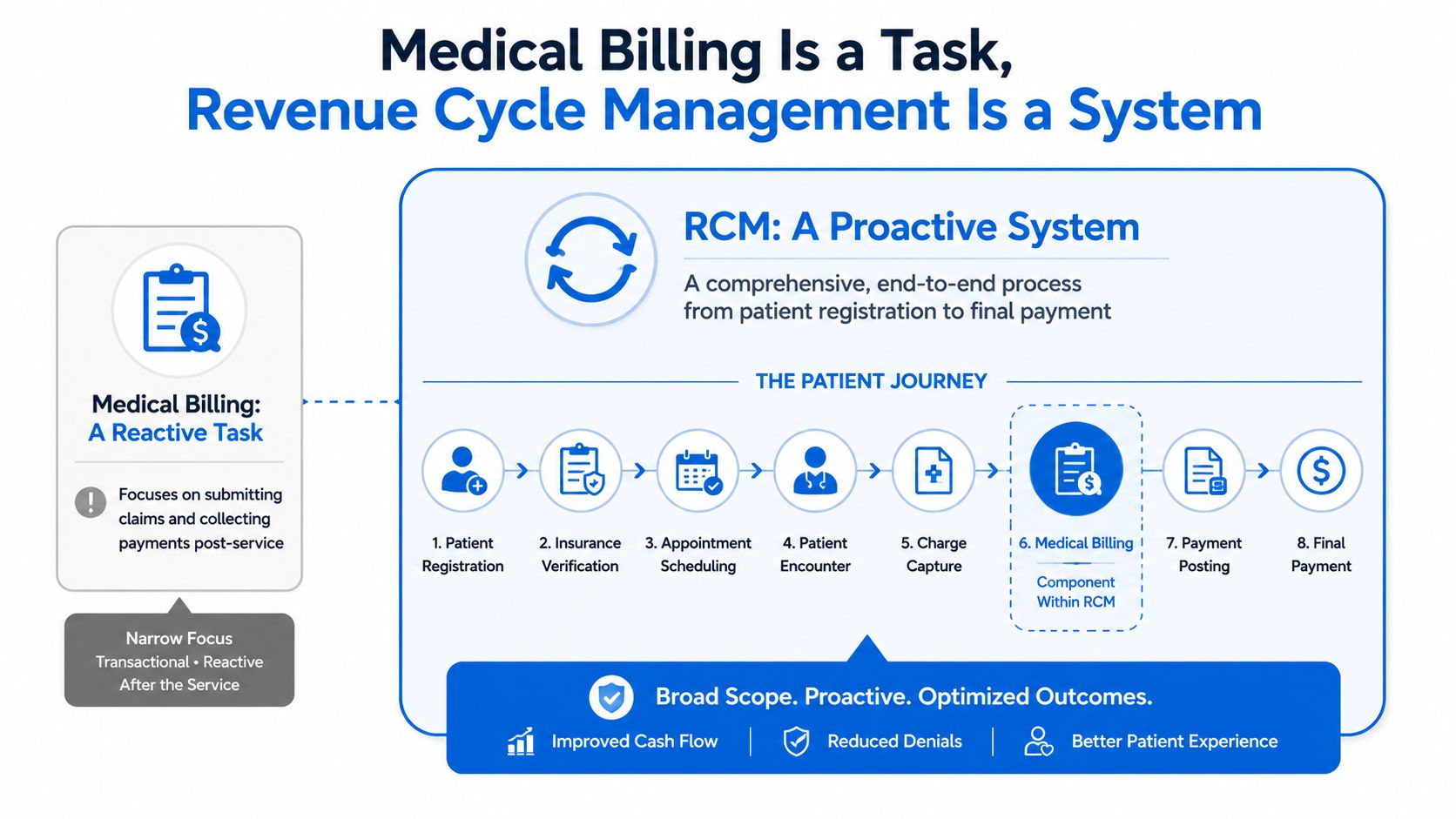
Medical billing is the execution layer. It handles the mechanics after care is provided. Revenue Cycle Management is the control system. It shapes the workflow before, during, and after the encounter so the claim has a better chance of being paid correctly the first time.
Why the scope difference matters
The clearest factual distinction is scope. Medical billing is a transactional subset of Revenue Cycle Management that typically handles only 30–40% of the total financial lifecycle, specifically stages 8 through 12, while RCM spans the full 13-step process from patient scheduling to revenue optimization and reporting, according to this breakdown of medical billing services vs Revenue Cycle Management.
That means billing usually starts after several high-risk moments have already passed. If registration data is wrong, benefits weren't verified properly, prior authorization was missed, or charge capture was incomplete, billing can only react. It can't go back in time and prevent the original error.
A useful way to explain medical billing vs Revenue Cycle Management to leadership is this:
- Medical billing is the claims office.
- RCM is the financial operating model for the entire patient encounter.
One processes transactions. The other governs performance.
What works and what doesn't
A billing-only setup can work when claims are straightforward, payer rules are relatively stable, and internal staff already manage front-end discipline well. That's a narrower environment than most practices operate in now.
What doesn't work is assuming the back office can compensate for weak intake, inconsistent authorizations, or coding drift. It can't. Those errors show up later as avoidable denials, slower cash conversion, and more staff time spent on rework.
Billing can tell you whether a claim was paid. RCM should tell you why claims get paid cleanly, why they don't, and what needs to change upstream.
Practices that understand that distinction stop treating reimbursement as a clerical process. They start treating it as an operational system with inputs, controls, and measurable outcomes.
Comparing Medical Billing and RCM Across Key Functions
Leaders usually don't need another abstract definition. They need to see how each model behaves in daily operations. That's where the difference becomes obvious.
An Early Comparison Table
| Function | Medical Billing | Revenue Cycle Management |
|---|---|---|
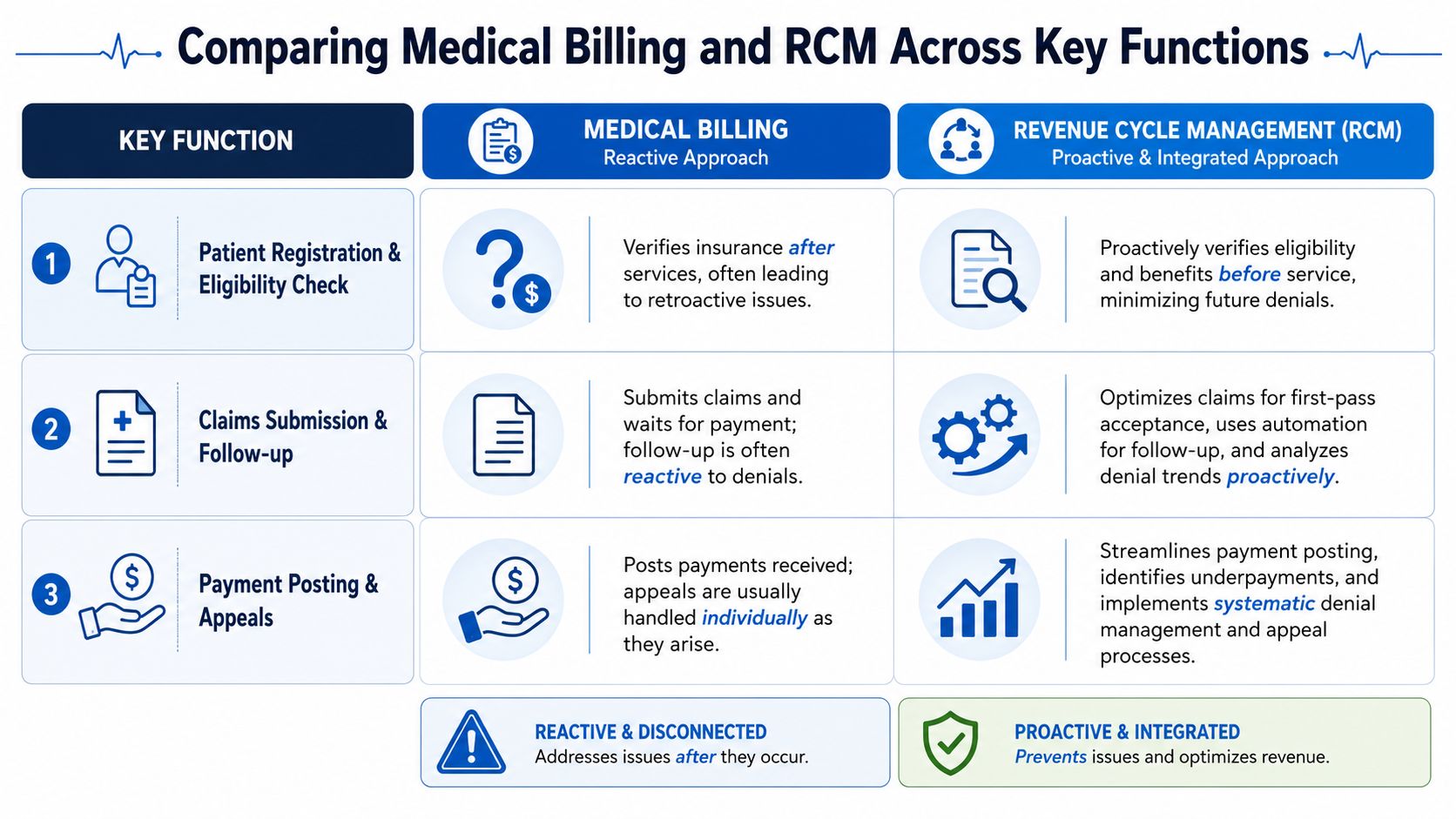
| Patient scheduling | Limited involvement | Integrated with financial workflow |
| Eligibility verification | Often checked at scheduling or check-in | Verified at scheduling and re-verified close to service |
| Prior authorization | Often outside core billing scope | Managed as part of pre-service controls |
| Charge capture | Receives charges after the fact | Monitors the process that produces accurate charges |
| Coding oversight | Focused on claim readiness | Connected to documentation quality and denial prevention |
| Claim submission | Core responsibility | Core responsibility, supported by upstream controls |
| Denial work | Reactive follow-up | Prevention, root-cause analysis, and appeals |
| Reporting | Queue-based status tracking | KPI-driven financial management |
| Leadership visibility | What got billed and what remains unpaid | Why revenue is delayed, denied, underpaid, or leaking |
Pre-service work changes the outcome
The most overlooked difference is pre-service discipline. In many billing-only arrangements, insurance is checked once during scheduling or at check-in. In full-cycle RCM, best-practice workflow verifies eligibility at scheduling and then re-verifies it within a 48-hour window prior to service. That matters because registration and eligibility failures drive 24.3% of all denials, according to these Revenue Cycle Management metrics.
That single operational distinction tells you a lot. Billing teams are often asked to rescue claims after payer rejection. RCM teams are built to prevent those rejections by tightening intake controls before the visit.
A related mid-cycle issue is charge capture. If the organization doesn't reliably turn documented care into complete, billable charges, clean claims become harder to achieve no matter how good the billers are. The process behind charge capture often exposes whether revenue leakage starts in documentation, coding handoff, or workflow design rather than in claim submission itself.
To ground the comparison in workflow, this short video is useful for leadership teams reviewing their current model.
Mid-cycle and post-service execution
Post-service is where medical billing is most comfortable. Claims go out. Payments are posted. Denials are worked. Patient balances are billed. That work is essential, but it's also where a billing-only model tends to stay trapped.
RCM adds two capabilities that billing teams often lack:
- Root-cause correction: not just reworking a denial, but identifying whether the denial came from intake, coding, payer edits, fee schedule setup, or contract variance.
- Performance management: not just aging receivables, but monitoring whether the process is trending toward cleaner claims and lower friction.
In practice, the side-by-side difference looks like this:
- Billing says: this claim denied for missing eligibility.
- RCM says: this payer and this location are producing the same eligibility error pattern, so the registration workflow needs to change.
That shift from task completion to system control is the operational divide.
Quantifying the ROI of Adopting Full Revenue Cycle Management
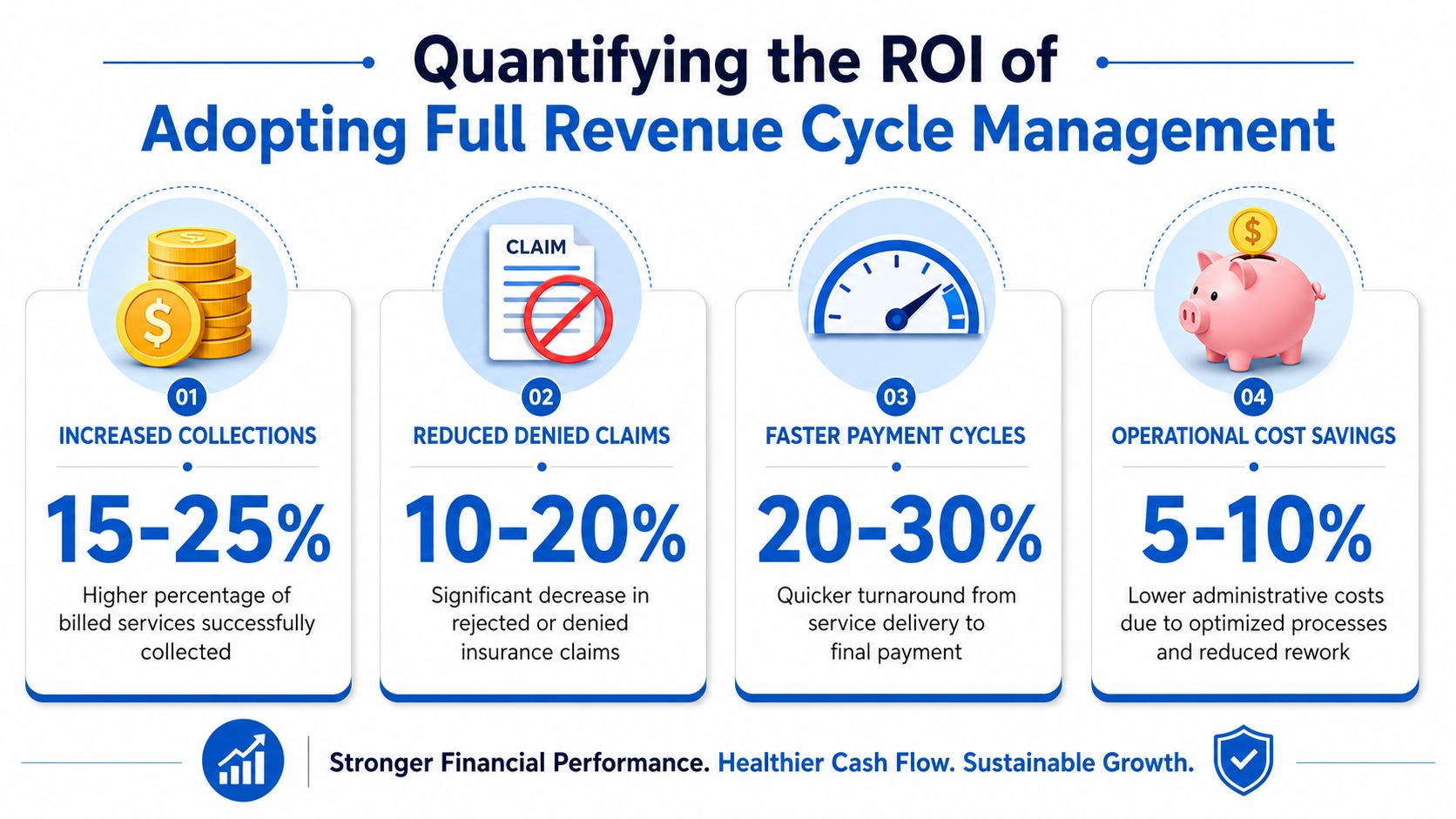
Healthcare leaders don't adopt full RCM because the concept sounds cleaner. They adopt it because the financial outputs improve when the operating model reduces preventable rework.
What the KPI gap actually means
The performance gap between billing-only and full RCM is large enough that leadership should treat the decision as a finance strategy issue, not an administrative preference. Organizations with full RCM see clean claim rates exceed 95%, net collection rates reach 98–99%, and average days in A/R drop below 30 days, compared to billing-only models where clean claim rates average 75–80%. The same source states that well-implemented RCM reduces administrative costs of billing and denial processing by 25–35% and increases cash flow by 20–30%, based on these essential medical billing KPIs for revenue cycle success.
For a leadership team, those aren't abstract metrics.
- Clean claims affect how much staff time gets consumed by avoidable resubmissions.
- Net collection rate reflects whether earned reimbursement is converting to cash.
- Days in A/R influences liquidity, forecasting accuracy, and how much pressure accumulates on working capital.
When those KPIs move in the wrong direction, the practice usually hires more people to chase the same dollars. That often masks the underlying issue. The process is producing too much rework.
Why finance teams care about this difference
A billing department can be busy and still underperform financially. Activity isn't the same as throughput. More calls, more appeals, and more follow-up notes can mean the organization is processing friction rather than removing it.
The strongest RCM programs don't win by working denials harder. They win by generating fewer avoidable denials in the first place.
That's the ROI case in plain terms. Better front-end controls create cleaner downstream execution. Cleaner execution reduces manual touches. Fewer manual touches lower administrative burden and accelerate payment.
For CFOs, that changes the conversation from “How many claims did the team submit?” to “How efficiently does the system convert care into cash?” That's the more useful number, even when it's measured through several KPIs rather than one headline metric.
Deciding Between In-House and Outsourced Financial Operations
Once leadership accepts that billing alone isn't enough, the next question is operational. Should the organization build a stronger Revenue Cycle Management function internally, outsource it, or run a hybrid model?
There isn't one answer for every practice. The right choice depends on staffing depth, payer complexity, specialty mix, reporting maturity, and how much management time leadership can dedicate to process oversight.
What stays difficult in-house
Many groups assume in-house means more control. Sometimes it does. It also means the organization must recruit, train, supervise, and retain people across multiple functions that don't sit neatly in one department. Front desk workflow, coding quality, denial management, payment posting, payer follow-up, and reporting all need coordination.
The harder problem is analytics. A billing office may know what's unpaid. That doesn't mean it can reliably identify why a pattern is repeating across payers, locations, or service lines. A 2024 report shows that 40% of practices fail to reduce denial rates over 3 years because billing teams lack analytics to pinpoint root causes, while RCM managers track KPIs to drive process improvement, according to this PMC report on healthcare financial operations and analytics.
That gap matters because most recurring revenue problems aren't single-claim issues. They're system issues.
When outsourcing makes operational sense
Outsourcing makes sense when leadership needs capabilities that are hard to build quickly in-house:
- Broader expertise: teams that have already seen payer behavior across multiple specialties and workflows.
- Technology access: reporting, work queues, and process monitoring that many smaller organizations won't build on their own.
- Scalability: the ability to absorb growth, turnover, or temporary backlogs without rebuilding the org chart.
- Focused accountability: one partner responsible for specific metrics, workflows, and escalation paths.
A hybrid model can also work well. Some practices keep internal registration or coding while outsourcing denial management, payment posting, or end-to-end medical billing services. That structure is useful when leadership wants to preserve existing staff strengths but close obvious process gaps.
The main mistake is choosing purely on headline cost. A cheaper billing arrangement that can't diagnose front-end leakage or reporting blind spots often becomes more expensive through missed revenue, rework, and delayed cash.
A Checklist for Choosing Your Financial Management Model
A practical decision starts with diagnosis. Most leadership teams already have enough information to tell whether they need a stronger billing process or a broader RCM model. They just need to ask better questions.
Questions leadership should ask now
Use these questions in your next finance or operations review:
Is our Clean Claims Ratio at or above the benchmark? The Healthcare Financial Management Association recommends aiming for a minimum 80% Clean Claims Ratio, according to this summary of RCM healthcare metrics. If you're below that threshold, the problem usually isn't just billing speed. It's process quality.
Can we identify our top denial causes with confidence? If your team can list denials only by volume and not by root cause, you're managing queues, not improving the system.
Does eligibility get verified once, or is it controlled as part of a repeatable pre-service workflow? A weak answer here usually points to front-end leakage.
Do front desk, coding, and billing leaders share the same KPI view? If each team reports in isolation, recurring losses are harder to trace and fix.
Do we know where underpayments occur? Many practices are good at spotting denials and weak at spotting partial reimbursement.
Are patient balances handled as part of a coordinated collection process? If statements go out but resolution is inconsistent, patient A/R will stay older than it should.
If leadership can't connect denied dollars to a specific workflow failure, the organization probably needs Revenue Cycle Management discipline, not just more billing labor.
This checklist isn't about forcing every practice into the same model. It's about exposing whether your current setup produces clarity or confusion. If answers are mostly operational and measurable, your process can likely be optimized. If answers are vague, fragmented, or team-dependent, the structure needs to change.
How Clarity Health RCM Delivers Comprehensive Financial Care
A full-service RCM partner should solve the exact gaps that billing-only models leave behind. That means more than claim submission and follow-up. It means managing the conditions that allow clean reimbursement to happen consistently.
Where a full-service partner fits
Clarity Health RCM provides support across the financial lifecycle, including fee schedule and practice management setup, billing operations support, insurance benefit verification, and claim status and payment posting. That scope matches the way leadership should think about medical billing vs Revenue Cycle Management. Billing remains a core function, but it performs better when eligibility, setup, and workflow controls are handled as connected parts of the same process.
For a practice that's struggling with denials tied to intake, payer mismatch, or inconsistent follow-up, that matters. The work doesn't start only when a claim drops. It starts where preventable revenue loss usually begins, in the operational handoffs before submission.
A full replacement or a targeted gap-fill
Not every organization needs the same engagement model. Some groups need an end-to-end operating partner because their internal structure can't sustain full-cycle discipline. Others already have capable internal staff and need targeted support in one or two weak areas.
That's why a customized approach usually works better than a blanket decision. A practice might need help with benefits verification and payment posting, while keeping internal oversight of coding and provider documentation. Another might want the full cycle managed externally so leadership can focus on provider operations instead of payer friction.
The useful starting point is a direct review of current workflows, reporting, and failure points. Once those are clear, the right model usually becomes obvious.
If your leadership team is weighing billing support against a broader Revenue Cycle Management strategy, Clarity offers a complimentary review of your current revenue cycle and can map either a full-service or a targeted solution based on the gaps you find.
No responses yet