The market itself tells you this isn't a back-office side issue. The U.S. healthcare revenue cycle management market was estimated at USD 172.24 billion in 2024 and is projected to grow at a 10.1% CAGR from 2025 to 2030, with the software segment projected to hold 79.65% of market share in 2026 according to Grand View Research's U.S. RCM market analysis. CFOs should read that for what it is. Healthcare RCM software has become core financial infrastructure.
Most buying guides still treat RCM software like a feature checklist. That misses the questions that determine ROI. First, can the system improve collections when more of the balance lands on the patient instead of the payer? Second, will the software integrate tightly enough with your EHR, front desk, coding, and denial workflows to matter, or are you just buying another dashboard?
If you're evaluating platforms, stop asking whether the tool “supports claims.” They all say that. Ask whether it reduces leakage before claim submission, shortens the path to cash, and helps staff collect the right amount from the right party with less rework. If it can't do that, it's not strategy. It's software spend.
Table of Contents
- Why Your Practice's Financial Engine Is Leaking Revenue
- What Healthcare RCM Software Really Is
- The Core Workflows Modern RCM Software Must Have
- Calculating the ROI of RCM Modernization
- A Framework for Evaluating RCM Software Vendors
- Navigating Integration Security and Compliance
- Taking Control of Your Revenue Cycle in 2026
Why Your Practice's Financial Engine Is Leaking Revenue
Practices do not lose revenue in one visible breakdown. They lose it in small failures that repeat all day. Eligibility is wrong at registration. Documentation reaches coding late. Claims leave with preventable errors. Patient balances arrive without a clear estimate, a clear explanation, or an easy way to pay. By the time the CFO sees the month-end numbers, the cash shortfall is already baked in.
That is why healthcare RCM software is getting more attention. Providers are not buying these systems for convenience. They are buying them because manual handoffs, disconnected tools, and weak patient payment workflows leave too much revenue exposed.
The leak is usually operational, and patient responsibility is now part of the problem
Many finance leaders start with payer contracts and fee schedules. Fair enough. But internal process failure often does more damage than a mediocre contract.
The biggest leak points usually look like this:
- Front-end errors: Incomplete registration and inaccurate insurance data create rework, denials, and slow collections.
- Missed or delayed charges: Weak handoffs between clinical documentation and billing delay cash and increase write-off risk.
- Poor claim quality: Claims sent without strong edits create denials your team should never have to touch.
- Weak patient collection flow: Staff ask for money too late, with poor estimates and disconnected payment options, so balances age out instead of converting to cash.
Patient responsibility has changed the math. More revenue now depends on whether your practice can estimate, communicate, and collect from patients before and after the visit. If your software handles payer billing well but treats patient collections like an afterthought, you still have a revenue leak.
If your teams still treat charge capture as a coding issue only, review how charge capture affects revenue integrity. The problem usually starts upstream in workflow design.
Practical rule: Treat RCM as a cash protection system, not an admin cost center.
Why CFOs should care now
The key decision is not whether to automate. It is where the value sits and where the risk sits.
Some practices get quick gains from point solutions. A stronger eligibility tool, better claim edits, or a cleaner patient payment product can improve one weak area fast. But point solutions also create more interfaces, more vendors, more support tickets, and more reconciliation work. End-to-end platforms reduce that friction, but only if the integrations with your EHR, scheduling, and payment systems work in practice, not just in the sales demo.
That is the CFO question. Can the software improve cash performance as patient balances rise, and can it do it without creating new integration failure points?
A practice can stay busy, submit a high volume of claims, and still underperform on cash because the revenue cycle runs as a set of disconnected tasks instead of one financial operating system.
What Healthcare RCM Software Really Is
Healthcare RCM software is the financial nervous system of a practice. It carries information from scheduling to final payment and makes sure each handoff supports reimbursement instead of damaging it.
That's why I don't like calling it billing software. Billing software creates claims. Healthcare RCM software should control the entire path to cash. It should tell your staff what to verify before the visit, what to collect at check-in, what's missing in documentation, which claims are risky, which denials deserve immediate action, and where patient balances are stalling.
It connects operations that usually live in silos
In many practices, the front desk, coding team, billers, and finance staff all work hard, but they work in separate systems. That creates lag, duplicate entry, and blind spots. A modern RCM platform should close those gaps.
At minimum, it should unify:
- Patient access tasks: Scheduling, registration, insurance verification, and financial clearance.
- Mid-cycle tasks: Charge capture, coding review, documentation support, and claim edits.
- Back-end tasks: Payment posting, denial routing, appeals, statements, and collections reporting.
When those workflows don't talk to each other, staff compensate manually. Manual compensation is expensive, slow, and inconsistent.
The right definition is operational control
A CFO shouldn't ask, “Does this vendor offer claims management?” That's too basic.
Ask better questions:
| Question | What a strong answer sounds like |
|---|---|
| Does it surface errors before submission? | The platform flags issues upstream, not after denial. |
| Does it connect to the EHR cleanly? | Eligibility, charges, and remits move with minimal manual intervention. |
| Does it support patient payments inside the workflow? | Estimates, balances, and payment collection aren't separate bolt-ons. |
| Does it give role-based visibility? | Front desk, billing, and finance each see what they need to act. |
A platform that only improves billing output is incomplete. The real value appears when registration, documentation, and collections all improve together.
What to ignore in vendor messaging
Ignore phrases like “AI-powered efficiency” unless the vendor can show where the intervention happens in the workflow. If the software doesn't clearly reduce front-end errors, organize work queues, and improve collection discipline, the language is decoration.
The useful distinction is simple. A basic tool automates tasks. A real healthcare RCM software platform improves financial control.
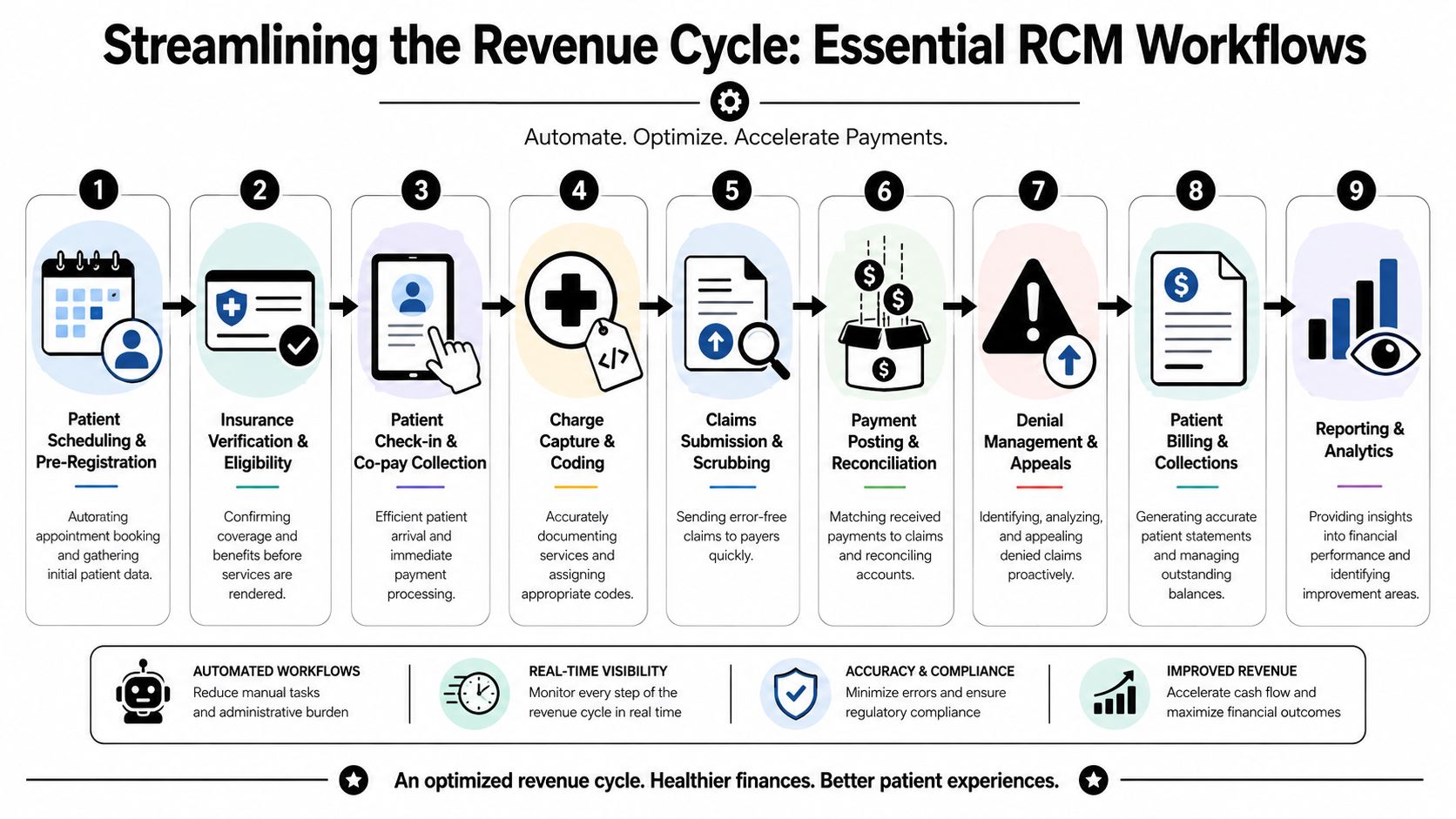
The Core Workflows Modern RCM Software Must Have
The best way to evaluate healthcare RCM software is to follow the money. Start at scheduling. End at cash posted and reconciled. If the platform breaks anywhere along that path, your staff will rebuild the process manually.
A complete system should handle the workflows below without forcing teams into disconnected tools.
Patient Registration and Eligibility Verification
Preventable denials either begin or are resolved.
Effective RCM software performs real-time eligibility verification that can confirm a patient's coverage, co-pay, and active status in seconds, and one implementation example reported a 28% decrease in eligibility-related denials after automated verification according to this healthcare RCM software development analysis. That's not a convenience feature. It's a front-end revenue protection function.
What good workflow looks like:
- Insurance checked before the visit: Staff don't wait until arrival to discover inactive coverage or benefit mismatches.
- Financial responsibility surfaced early: Co-pays and patient obligations are visible while the patient can still act on them.
- Exceptions routed intelligently: Staff focus on unresolved accounts instead of rechecking everyone manually.
Charge Capture and Medical Coding
A claim can't be cleaner than the documentation and charges feeding it. If providers document late or coders work from incomplete notes, the revenue cycle slows immediately.
Strong platforms reduce friction between clinical activity and financial capture. They don't replace coding judgment. They make the handoff cleaner and faster.
Look for systems that support:
- charge review tied closely to documentation,
- coding workflow visibility by provider or location,
- work queues for missing or incomplete encounters.
A practice can outsource parts of this process too. For example, Clarity provides medical coding and billing support for healthcare revenue cycle workflows, along with patient account and credentialing support, which can help practices fill operational gaps without replacing every internal process at once.
Claims Submission and Scrubbing
Claim generation without editing is just denial creation at scale.
Your platform should scrub claims before they leave the system, apply payer-specific edits where possible, and show staff exactly what needs correction. That reduces rework and protects first-pass performance.
Teams that want deeper visibility into claim quality trends should also monitor healthcare revenue cycle analytics rather than relying on end-of-month summary reports alone.
A strong claims workflow does three things well:
- catches missing or invalid data before submission,
- routes exceptions to the right user quickly,
- tracks claim status without forcing staff into payer portal chaos.
Here's a useful explainer on the broader process:
Denial Management and Appeals
Most denial workflows fail because they're reactive. Staff work the loudest accounts first, not the most recoverable ones. They chase payer issues one by one instead of identifying patterns.
Modern RCM software should categorize denials, route them by root cause, and support appeals inside the same operational flow. If the system can't tell you whether denials originate from eligibility, coding, documentation, or payer edits, your denial process is still mostly manual, even if it looks digital.
Denials should be managed as a pattern problem, not an inbox problem.
Payment Posting and Reconciliation
Payment posting gets less attention than claims, but it's where finance discovers whether expected cash was received.
The software should post remits efficiently, reconcile payer and patient payments against expected amounts, and surface underpayments or mismatches for review. If staff need multiple systems and spreadsheets to understand cash application, the platform isn't finished.
This workflow matters because it closes the loop. Without clean reconciliation, your reporting is unreliable and your A/R prioritization is weaker than it looks.
Reporting and Analytics
Dashboards don't create ROI. Actionable visibility does.
A useful reporting layer should show:
- Where cash is stalling: by payer, provider, location, and aging bucket.
- Which denials repeat: by category and root cause.
- How front-end performance affects collections: especially registration accuracy and financial clearance.
- What patient balances are doing: not just payer A/R.
If the analytics only summarize the past, they're accounting. If they help staff intervene earlier, they're operations.
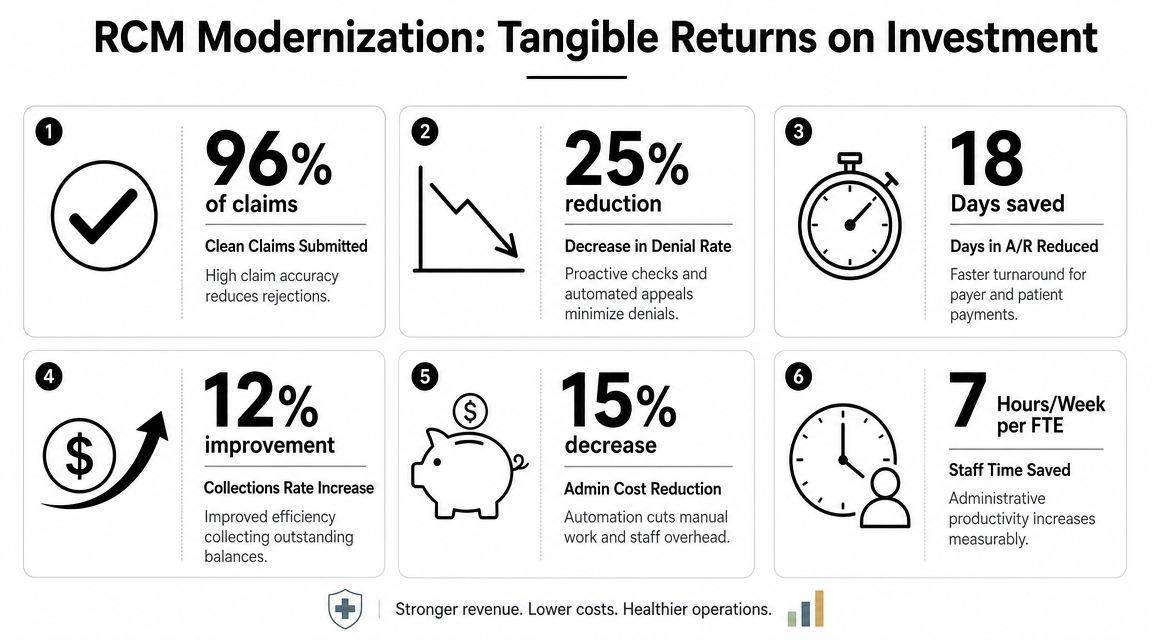
Calculating the ROI of RCM Modernization
CFOs shouldn't buy healthcare RCM software because it sounds efficient. They should buy it when the numbers and workflow changes support a clear financial case.
The pressure is already obvious. Industry benchmark reporting notes that 5% to 10% of healthcare claims are denied annually, that nearly 41% of providers reported denial rates of at least 10% on submitted claims, and that the financial impact of denials reaches up to USD 262 billion annually. The same benchmark set points to operational targets such as above 95% clean claim rates, 95% to 99% net collection rates, and 30 to 40 days in accounts receivable according to this revenue cycle management statistics summary. Those aren't vanity metrics. They're the baseline for evaluating whether your current process is underperforming.
The KPI Set That Actually Matters
Don't let vendors steer the conversation toward logins, automation counts, or how many rules sit in the engine. The finance team should stay focused on five outcomes.
- Clean claim rate: If edits and scrubbing work, more claims go out correctly the first time.
- Denial rate by root cause: You need to know whether the lift comes from better eligibility, coding, documentation, or payer follow-up.
- Days in A/R: Cash timing matters. Slow collections tie up working capital fast.
- Net collection rate: This is one of the clearest indicators of how much collectible revenue you're converting. If your team needs a refresher, this guide on net collection rate in healthcare billing is worth reviewing.
- Patient collection performance: Rising patient responsibility means payer metrics alone no longer tell the full story.
Where Patient Payment Workflow Changes the Math
Many RCM projects disappoint by automating claim flow but ignoring the patient's side of the balance.
As patient responsibility rises, your software needs to do more than send statements faster. It should support front-end eligibility accuracy, clearer patient estimates, point-of-service collection, and a billing experience that doesn't create more confusion than payment. If automation shifts work from your staff to the patient, you may speed up billing while hurting actual collections.
A practical way to assess ROI is to ask where dollars are currently delayed or lost:
| Revenue issue | What the software should change |
|---|---|
| Eligibility-related denials | Verification before service and exception routing |
| Dirty claims | Pre-submission edits and payer-aware scrubbing |
| Slow collections | Better work queues, posting, and follow-up visibility |
| Weak patient payment performance | Better estimate quality, easier payment flow, earlier collection touchpoints |
If a vendor can't explain how its workflow improves patient collections, not just payer reimbursement, the ROI model is incomplete.
The smartest CFOs don't approve RCM software on faith. They model expected improvement in denial prevention, cash timing, and net collections, then tie implementation milestones to those outcomes.
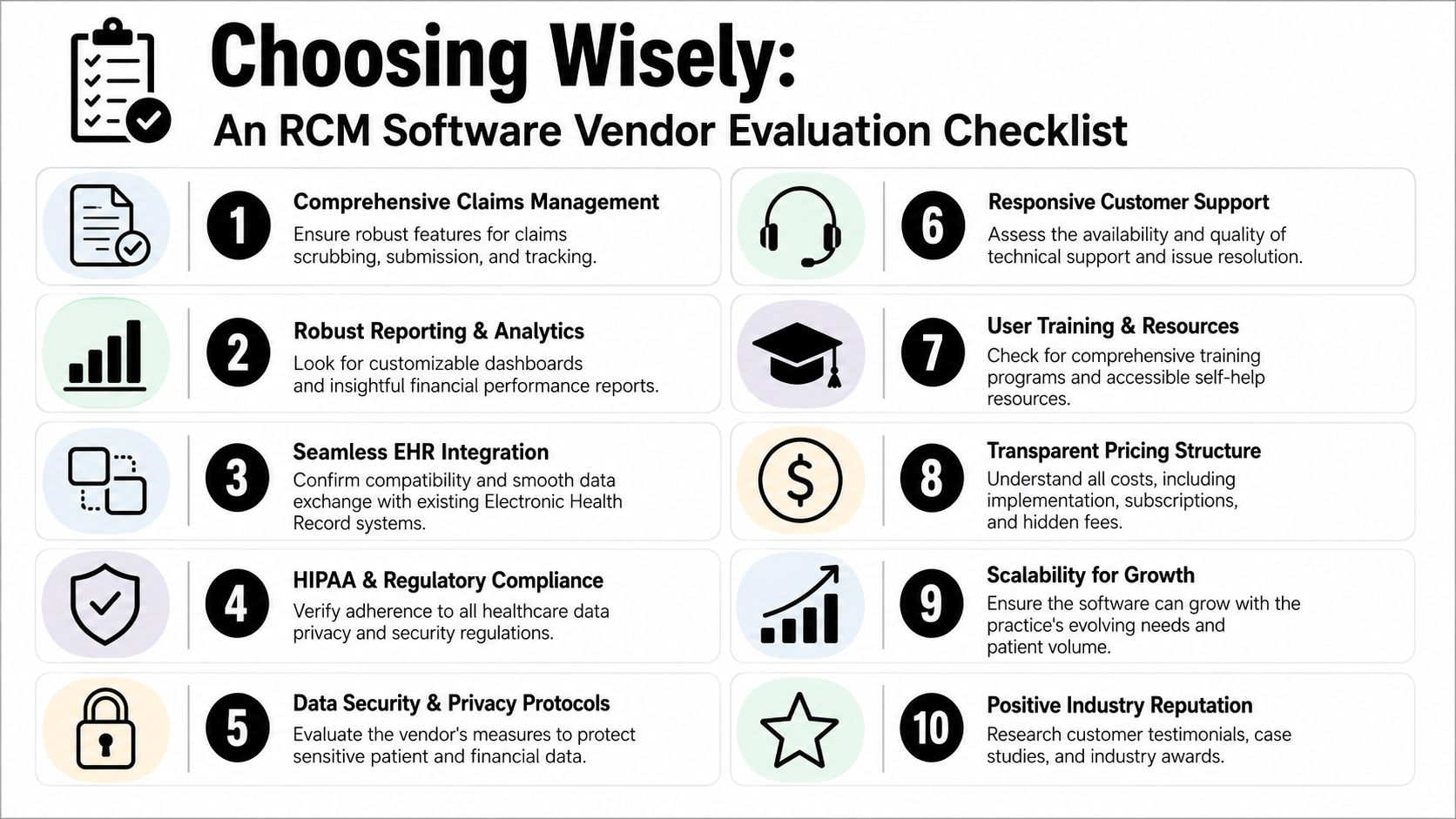
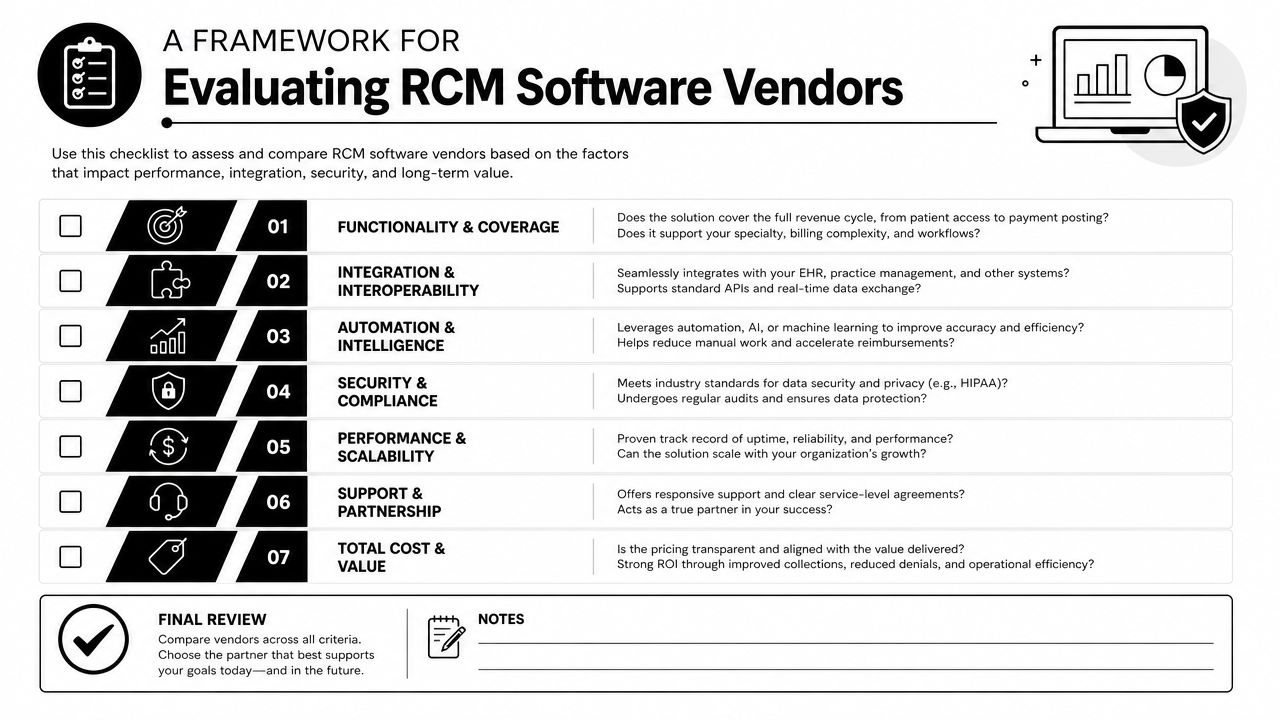
A Framework for Evaluating RCM Software Vendors
Most vendor evaluations fail because the shortlist is built on demos, not operating reality. Everyone shows a polished claim screen. Everyone says they integrate. Everyone promises cleaner workflows. The decision is whether you want a point solution that fixes one painful task or an end-to-end platform that changes how revenue moves across the practice.
That distinction matters more than feature count.
Point Solution Versus Connected Platform
Independent analysis on the category makes the strongest argument clearly. Much of the ROI opportunity often comes from integrated, multi-product workflows that connect patient onboarding, documentation, and denials, and buyers should ask whether a vendor is selling a billing tool or a fully connected platform because integration depth can matter more than feature count in a crowded market, as argued in this analysis of the healthcare RCM opportunity.
Here's the blunt version. Point solutions are attractive because they seem easier to buy. They solve one visible problem, usually eligibility, claims editing, or denials. But they often create a second problem. Your team now has another system, another queue, another vendor, another interface, and another set of data handoffs to manage.
End-to-end platforms have the opposite risk. They can realize more value, but only if implementation is disciplined and the EHR connection is real.
A side-by-side view helps:
| Model | Good fit | Main risk |
|---|---|---|
| Point solution | You have one severe bottleneck and strong existing systems elsewhere | Workflow fragmentation |
| Integrated platform | You need cross-functional improvement and better financial visibility | Longer implementation and adoption curve |
| Hybrid approach | You want to keep core systems and add targeted layers carefully | Integration governance becomes critical |
Questions to Force a Straight Answer in Demos
Don't ask vendors what features they offer. Ask what work disappears for your staff.
Use questions like these:
- Where does the platform sit relative to the EHR? If the answer is vague, integration risk is high.
- What happens when eligibility fails, documentation is incomplete, or a denial appears? You want workflow routing, not generic assurance.
- How does patient payment fit into the same system? If estimates, balances, and payment options live elsewhere, friction stays high.
- Which workflows are configurable by payer, location, or specialty? Rigid systems create workarounds.
- What does implementation require from our internal team? If the vendor minimizes this, expect surprises later.
Buy the workflow, not the screenshot.
The strongest vendor isn't the one with the most modules. It's the one whose integration model matches how your practice operates.
Navigating Integration Security and Compliance
Most RCM software projects don't fail because the software lacks features. They fail because the implementation team underestimates workflow disruption.
Integration Failure Usually Starts in Workflow Design
If your EHR, scheduling, billing, and payment processes already conflict, new software will expose the problem fast. It won't hide it. Before rollout, finance and operations need agreement on ownership of key events: registration accuracy, eligibility exceptions, charge lag, claim edits, denial routing, patient balance communication, and payment posting review.
A practical rollout checklist should include:
- Data handoff mapping: Know exactly where patient, insurance, charge, and remit data originate and where they land.
- Exception ownership: Assign who resolves failed eligibility, claim edit failures, coding holds, and denial work queues.
- Cutover discipline: Don't switch workflows midstream without clear reconciliation rules.
Security and Adoption Are Operational Issues
HIPAA and data security aren't procurement checkboxes. They affect daily operations. Your team should understand access controls, audit visibility, user roles, and what happens when data crosses systems or vendors. If the platform touches patient balances, remits, and insurance details, finance should care as much as IT does.
Training matters just as much. The best healthcare RCM software still underperforms if front-desk staff bypass verification steps, coders work outside the queue, or billers maintain shadow spreadsheets because they don't trust the reporting.
Good implementation reduces side work. If staff create parallel processes after go-live, something is broken.
Adoption is your final integration test. If users can't follow the new workflow consistently, the projected ROI won't show up in cash.
Taking Control of Your Revenue Cycle in 2026
A small breakdown in collections, denials, or patient balance follow-up can erase margin faster than most cost cuts can recover it. That is why healthcare RCM software belongs in the CFO's operating plan, not on a generic IT shopping list.
In 2026, the decision comes down to two questions. First, how well does the system handle rising patient financial responsibility before and after the visit? Second, where will value come from in your environment: a stronger point solution for a specific bottleneck, or an end-to-end platform that reduces handoffs, duplicate work, and reporting blind spots?
Start with your cash problems, not the demo.
Review where self-pay balances stall, where staff lose time chasing avoidable denials, and where integration gaps force teams to rekey data or work outside the system. If a vendor cannot show how patient estimates, payment collection, claim status, denial follow-up, and posting reconcile across the workflow, you are buying more complexity.
Use a short decision checklist:
- Pressure-test patient collections: Review how the software supports estimates, pre-service collection, payment plans, statements, text-to-pay, and follow-up on high-balance accounts.
- Identify integration risk: Ask what breaks when eligibility, PM, EHR, clearinghouse, and payment data fall out of sync, and who owns the fix.
- Choose platform vs point solution based on leakage: Buy a point solution if one failure point is driving losses. Choose a broader platform if handoffs and fragmented reporting are the bigger problem.
- Tie the purchase to finance metrics: Set targets for net collection rate, days in A/R, denial rate, patient collection yield, and staff work per claim.
The best choice is the one that gives finance cleaner visibility, operations tighter process control, and patients a clearer path to pay.
If you want an outside view before committing to software or redesigning internal workflows, Clarity offers a complimentary consultation on your current revenue cycle. That can help you identify where denials, collection friction, and process gaps are undermining financial performance before you invest in a new platform or expand your existing stack.
No responses yet