
15% more cash collected on average and a 90% denials overturn rate is the kind of result R1 RCM reports for AR recovery work, which should change how most finance leaders think about receivables. This isn't back-office cleanup. It's a cash acceleration function tied directly to margin, forecasting, and write-off prevention when old balances are still recoverable through R1 RCM's AR Recovery service.
For healthcare CFOs, the harder question isn't what AR recovery is. It's where to deploy it, how to scope it, and when a legacy cleanup project still makes economic sense. Routine follow-up and true old-AR remediation are not the same job, and treating them as one usually wastes labor on claims that need a different playbook.
Table of Contents
- The High Cost of Uncollected Revenue in Healthcare
- What Are Healthcare AR Recovery Solutions
- The AR Recovery Workflow and Key Metrics
- Building the Business Case for AR Recovery
- How to Implement an AR Recovery Strategy
- Taking Control of Your Revenue Cycle in 2026
The High Cost of Uncollected Revenue in Healthcare
In healthcare, AR is money already earned but not yet collected. That distinction matters. Once a balance starts aging, the issue stops being accounting hygiene and becomes a rising risk to cash flow, denial exposure, and eventual write-off.
The industry has already moved away from paper-heavy billing and manual follow-up toward claims automation and analytics because delayed receivables create financial pressure fast. Current operating guidance emphasizes fast submission, payer-specific claim scrubbing, portal-based status tracking, denial analytics, and aging reports that push teams toward the balances most worth pursuing, as described in this healthcare AR recovery overview.
That shift changed what “good AR management” looks like. It's no longer enough to post charges, send claims, and wait for remits. Strong AR control starts earlier.
Three controls that protect cash
- Eligibility before service: Verification reduces preventable downstream rework and keeps the claim from entering AR with obvious defects.
- Clean claims fast: Claims need to go out quickly and in payer-compliant form. Delay shortens the time available for correction, appeal, and collection.
- Structured aging follow-up: Teams need work queues, escalation rules, and ownership by payer and denial type.
Practical rule: If a claim reaches aging buckets before anyone identifies the root cause, recovery gets more expensive because every later touch requires more labor and usually better documentation.
A CFO should also look upstream. Weak front-end processes create AR problems that recovery teams inherit later. If charge capture is inconsistent, the billing office starts with the wrong inventory. That's why many organizations review AR strategy alongside charge capture workflows in healthcare.
Why older balances cost more to recover
Not every aged account is merely “late.” Some are drifting because of authorization gaps, missing documentation, payer edits, bad registration data, or unresolved patient responsibility. Each category calls for different action. Uniform follow-up scripts don't fix structurally different problems.
That's the first strategic takeaway. AR recovery solutions create the most value when leadership treats receivables as a segmented asset, not a single aging report.
What Are Healthcare AR Recovery Solutions
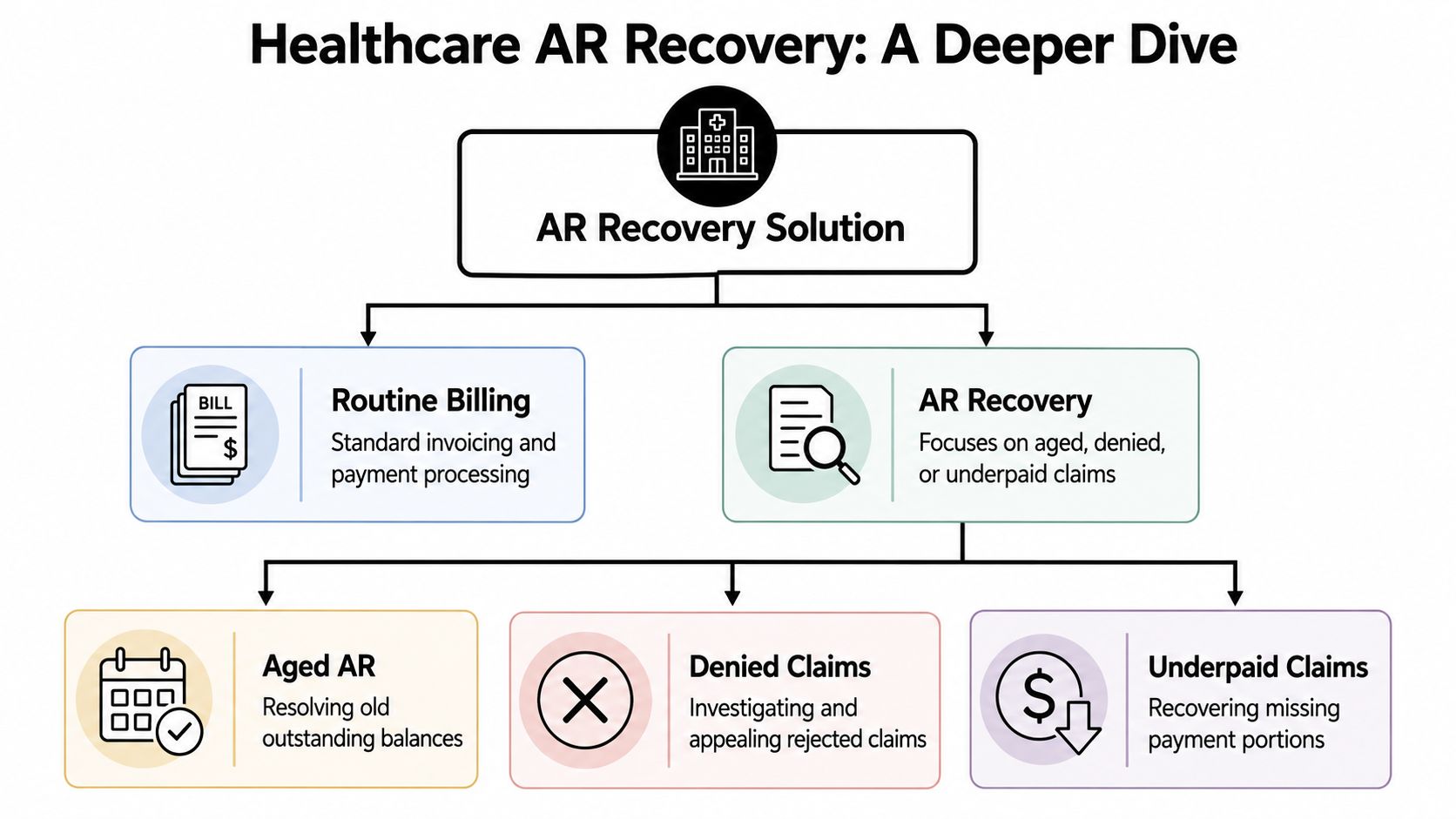
AR recovery solutions are the systems, workflows, and specialist labor used to pull revenue back from aged, denied, underpaid, or otherwise stalled claims. Routine billing handles the normal path from charge entry to payment posting. Recovery steps in when claims fall out of that path and need targeted intervention.
Used well, AR recovery functions like a financial ICU for claims that won't resolve through standard queues.
Routine AR is not the same as recovery
A lot of buyers blur these together. They shouldn't.
Routine AR work usually includes status checks, standard follow-up, payment posting coordination, and ordinary payer communication. Recovery work is different. It focuses on accounts that are already off the happy path and often need one or more of the following:
- Denial rework: Correcting root causes, preparing appeal packets, and resubmitting within payer rules.
- Underpayment review: Identifying balances where payment posted but the account still needs adjudication or contractual review.
- Patient balance resolution: Working balances that require cleaner statements, better categorization, or coordinated follow-up after payer exhaustion.
- Aged claim escalation: Pulling older receivables into dedicated work queues instead of letting them sit in general AR.
The operational mindset changes too. In standard billing, volume and timeliness dominate. In recovery, judgment matters more. Teams have to decide which claims are worth pursuing, which need documentation repair, and which should move to controlled closure.
AR recovery works best when teams stop asking, “Was this claim touched?” and start asking, “What is preventing payment, and is that obstacle still solvable?”
Legacy AR needs its own scope
Many organizations lose money. Old AR isn't just routine AR that nobody got to yet. Some balances are structurally hard to collect because they're tied to EMR migrations, incomplete documentation, staffing turnover, payer recoupments, or orphaned balances. Vendors often distinguish ordinary AR work from cleanup projects for exactly that reason, as noted in this review of AR run-down and recovery audits.
That distinction is important for budgeting and staffing. A cleanup project usually needs:
| AR type | Typical issue | Best approach |
|---|---|---|
| Current routine AR | Ordinary follow-up and status lag | Standard team workflows |
| Aged AR | Claims sitting unresolved too long | Dedicated recovery queues |
| Legacy cleanup AR | Migration, documentation, or ownership problems | Project-based triage and scoping |
| Denied complex AR | Appeals and medical necessity disputes | Specialist review |
A cleanup engagement should begin with segmentation, not promises. Separate claims by age, payer, denial category, data completeness, and documentation availability. Then decide what belongs in active recovery, what requires a one-time project team, and what isn't economically rational to keep touching.
What good AR recovery solutions include
The strongest programs usually combine process discipline with targeted tools.
- Work queues by age and value: High-dollar, high-probability claims should not compete with low-balance noise.
- Denial category routing: Medical necessity, eligibility, coding, authorization, and documentation failures rarely belong with the same staff.
- Appeal and resubmission controls: Teams need a repeatable method for gathering records, correcting claims, and tracking payer responses.
- Management reporting: Finance needs visibility into cash recovered, balances remaining, and where claims are still getting stuck.
Service models often diverge significantly. Some firms offer only overflow follow-up. Others can handle segmented cleanup, legacy run-down, and ongoing prevention work. Those are different buying decisions, and a CFO should scope them separately.
The AR Recovery Workflow and Key Metrics
AR recovery becomes effective when it runs as an operating system, not a loose collection of follow-up tasks. The strongest teams use a structured workflow that moves claims from identification through resolution and then back into reporting that finance can act on.
A practical operating model
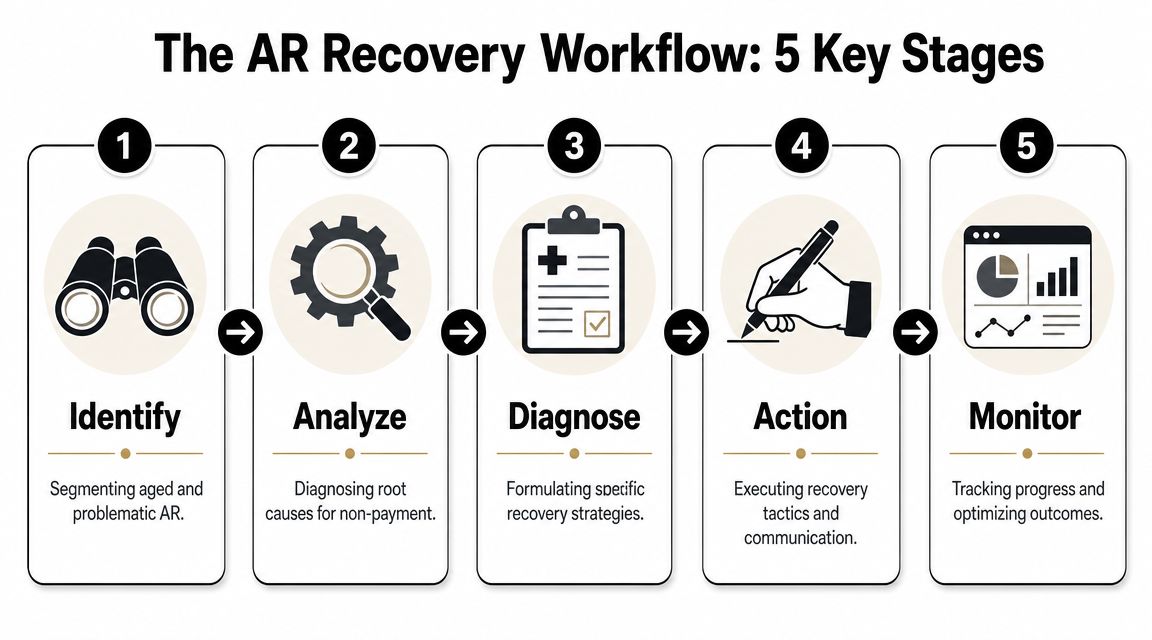
A simple five-stage model works well in practice.
Identify
Pull the AR population apart by age, payer, denial status, balance size, and documentation readiness. Through this analysis, teams isolate the claims that need recovery rather than ordinary billing attention.Analyze
Determine why payment stalled. Some claims need corrected demographics. Others need appeal logic, medical records, or a payer escalation.Diagnose
Choose the right tactic for each segment. One set of claims may justify immediate appeal. Another may need rapid resubmission. A third may need controlled closure if records are incomplete.
Before moving further, it helps to align the operations team around the workflow visually.
Action
Work the claims through payer portals, call queues, appeal submissions, patient balance processes, and internal correction loops.Monitor
Track outcomes by segment, not just in aggregate. If one payer category absorbs labor with low yield, the team should know quickly.
Aging segmentation is central here. One AR recovery service identifies the 60-to-120+ day aging window as the threshold for targeted cleanup, which reflects how modern teams segment delinquency by time since service rather than treating every balance the same way, according to Medcare MSO's AR recovery framework.
What finance leaders should measure
Many executive dashboards still overemphasize gross billed charges or call volume. Those metrics don't tell you whether recovery work is producing cash.
The better lens includes these measures:
- Aging days: How much of the inventory sits in older buckets that need focused attention.
- Recovery percentage: What share of targeted AR produces actual collections or balance resolution.
- Denial turnaround time: How quickly the team moves from denial identification to appeal, correction, or closure.
Operator's view: A high-touch team can still underperform if touches aren't matched to the right denial categories and payer deadlines.
Finance also needs reporting that joins operational detail to financial outcome. That means looking beyond aging totals and using healthcare revenue cycle analytics to compare payer performance, denial categories, work queue yield, and claim resolution speed.
Metrics that help with hard cleanup decisions
Legacy AR creates a different management problem. The key question is not “How much is still outstanding?” It's “What portion of this inventory is actionable at an acceptable labor cost?”
A short decision table helps:
| Metric | Why it matters |
|---|---|
| Age bucket | Older claims usually need stronger prioritization and more selective effort |
| Balance size | Small balances can consume too much labor if handled manually |
| Denial category | Some categories justify appeals. Others are poor recovery candidates |
| Documentation status | Missing records can turn a collectible balance into a cleanup write-off |
| Payer response speed | Slow or opaque payer processes change the labor equation |
If a vendor can't show this level of segmentation, you're not buying a recovery engine. You're buying extra follow-up labor.
Building the Business Case for AR Recovery
A large AR balance does not automatically justify a recovery project. The business case has to show incremental cash after labor, vendor fees, and write-off acceleration. For a healthcare CFO, the question is straightforward: which parts of the inventory will produce cash at a return that beats other uses of staff time and operating expense?
Earlier benchmarks from R1 RCM point in the same direction. Recovery performance improves when teams sort claims by recoverability, denial type, documentation status, and payer behavior. It does not improve just because more accounts get touched.

The ROI case starts with scope, not effort
The strongest business cases begin with segmentation. Separate routine aging from true legacy cleanup, then isolate the inventory that has a realistic path to payment. That keeps the organization from spending senior analyst time on claims that are too old, too small, or too poorly documented to justify active follow-up.
A practical finance model usually tests three areas:
- Recoverable cash in the current inventory: Identify balances that are denied, stalled, or aging but still workable under payer rules and filing limits.
- Internal capacity released for higher-value work: AR teams often burn hours on low-yield status checks because no one narrowed the inventory first.
- Future loss reduction: Root-cause findings from recovery work can reduce repeat denials, missed rebills, and avoidable write-offs.
That is why AR recovery should be evaluated alongside broader medical revenue recovery strategies. A cleanup project is not just a collections exercise. It is also a diagnostic tool for finding the process failures that created the backlog.
Where weak business cases fail
The weakest proposal says, “We have old AR, so we need more people.” That approach usually increases touches, extends the life of bad inventory, and creates little measurable lift in cash.
A stronger case asks harder questions before any staffing decision is made:
| Weak assumption | Better finance question |
|---|---|
| All old AR is collectible | Which segments still have enough yield to cover labor and appeal cost? |
| More follow-up creates more cash | Which denial categories actually convert after correction or appeal? |
| One team can work the whole backlog | Which segments need specialists, and which should be closed quickly? |
| Legacy AR is just delayed routine work | Is the inventory tied to a conversion, staffing gap, documentation failure, or payer-specific dispute pattern? |
That last question matters more than many leadership teams expect. Legacy cleanup projects behave differently from normal AR management. The workflow is less predictable, the documentation gaps are larger, and the staffing model often needs a temporary project structure with tighter QA and faster escalation paths.
The real trade-off is yield versus labor
Many organizations often either overbuild or underinvest.
If the backlog contains high-balance claims with workable denials and available records, a focused recovery effort can produce a clear return. If the inventory is dominated by small balances, missing documentation, expired filing windows, or payer classes with poor overturn history, the financially sound decision may be faster closure and cleaner write-offs. Both outcomes can improve the balance sheet. The difference is whether leadership is choosing based on segmented yield data or on hope.
Financial test: If a proposal cannot show expected cash recovery by aging band, balance tier, denial category, and labor model, it is not a business case. It is a staffing request.
A mature case also separates one-time cleanup economics from steady-state operations. Routine AR should be measured on sustainable performance inside the revenue cycle. Legacy AR should be measured as a scoped project with a defined inventory, timeline, recovery target, and closure plan. Mixing those two models usually hides both the true ROI and the true write-off risk.
How to Implement an AR Recovery Strategy
Implementation starts with a strategic choice. Should you build a dedicated in-house capability, or should you use an outside partner for some or all of the work? The answer depends less on ideology and more on claim complexity, staffing depth, payer mix, system fragmentation, and whether you're dealing with routine aging or a hard cleanup project.
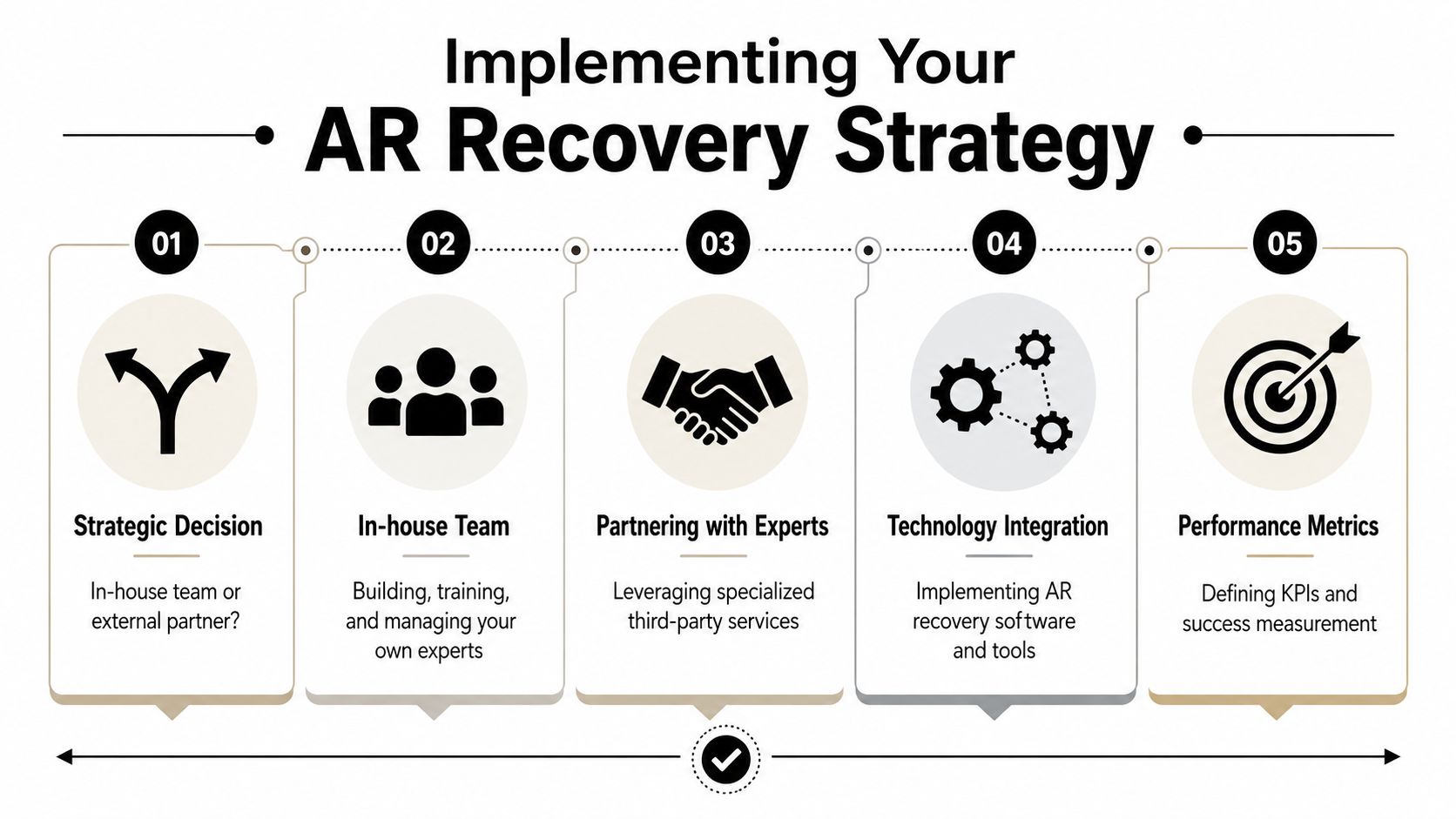
In-house versus outsourced
An internal team gives you direct control. That matters when payer issues are tightly tied to your front-desk workflows, coding patterns, or physician documentation habits. Internal staff often know the local process failures better than any outside vendor can.
External support makes sense when the backlog is specialized, when staffing is thin, or when the organization needs project-based cleanup capacity without building it permanently. Some providers, including Clarity, offer modular RCM support that can cover benefit verification, claim status work, payment posting, and targeted billing functions rather than requiring a full platform handoff.
Here's the practical comparison:
| Model | Strength | Limitation |
|---|---|---|
| In-house team | Direct control, easier alignment with internal workflows | Harder to scale for cleanup spikes or specialty denials |
| Outsourced recovery partner | Faster access to specialized labor and segmented workflows | Requires tighter oversight, reporting, and governance |
| Hybrid model | Keeps strategic control while outsourcing hard segments | Needs clear ownership rules to avoid duplication |
A vendor checklist that actually matters
Technology fit is one of the first screening questions. An effective AR recovery workflow should integrate with the current billing environment through HL7/FHIR and ANSI X12 standards so teams can automate status checks and follow-up without replacing the practice management platform, which reduces errors and shortens resolution time according to Dastify's medical billing AR recovery overview.
That means a vendor conversation should move quickly past generic claims and into specifics.
Ask questions like these:
- Integration capability: Can the team work inside your current PM, clearinghouse, and EHR environment, or will they force side systems and spreadsheet handoffs?
- Segmentation discipline: How do they divide routine AR, aged AR, denied claims, underpayments, and legacy cleanup inventory?
- Payer expertise: Do they show payer-specific workflows, or do they rely on generic call-center follow-up?
- Legacy project design: How do they handle migration-related balances, incomplete records, and orphaned accounts?
- Reporting clarity: Will finance receive segmented reporting by age, denial type, recovery status, and cash impact?
- Operational governance: Who owns corrections, appeals, patient follow-up, and closure decisions?
Don't hire a recovery partner based on dashboards alone. Hire one based on how clearly they define claim ownership, escalation paths, and closure criteria.
What to do before go-live
Even strong vendors fail when implementation starts with bad inventory and vague ownership.
A solid launch plan usually includes:
Freeze the scope
Define whether the engagement covers current aged AR, denials, underpayments, legacy cleanup, or some combination.Create segmentation rules
Decide which claims stay with internal staff and which move to the recovery team.Agree on closure logic
Teams need rules for when to appeal, when to resubmit, when to escalate, and when to stop.Set management reporting early
Finance should review recovery by segment, not just total collections.Feed findings upstream
Recovery only creates long-term value if repeated failure modes are sent back to registration, coding, authorizations, and claim editing.
Implementation becomes strategic. Good AR recovery solutions don't just drain the backlog. They help prevent the next one.
Taking Control of Your Revenue Cycle in 2026
The most useful way to think about AR recovery in 2026 is as a targeted capital allocation decision inside the revenue cycle. You are deciding where specialized labor, analytics, and management attention will produce the most collectible cash. That's very different from treating AR as a generic back-office burden.
The organizations that get the best results usually do three things well. They separate routine billing from recovery work. They segment aged and legacy inventory before assigning labor. And they measure success by cash, aging movement, and denial resolution speed rather than by raw activity.
That last point matters. A large aging report can create false urgency. Some balances deserve rapid escalation. Some belong in a one-time cleanup project. Some should be closed with discipline because the cost to pursue them no longer makes sense. Strategic AR recovery is about making those distinctions early.
The operating posture that works
- Protect the front end: Eligibility, authorizations, and clean claim submission still do more for margin than heroic cleanup later.
- Triage the backlog: Not all aged claims are equal. Work them by recoverability, value, and documentation readiness.
- Use recovery as feedback: If the same denial patterns keep appearing, the problem is not AR. The problem is process design upstream.
Old AR is often a symptom. The deeper issue is usually inconsistent ownership between front-end intake, claim editing, denial management, and payment resolution.
For CFOs, the next step isn't another generic AR meeting. It's an honest assessment of current inventory. How much of your backlog is ordinary delay, how much is denial-driven, and how much is legacy AR that needs a cleanup strategy of its own? Once those buckets are clear, the right staffing model and technology approach become much easier to choose.
Clarity offers a complimentary review of your current revenue cycle and can help assess whether your backlog calls for routine follow-up support, targeted AR recovery, or a scoped legacy cleanup plan. If you want a practical read on where cash is stuck and what actions are worth taking, you can start with Clarity.
No responses yet