The number that should get a CFO's attention isn't a staffing ratio or a software feature list. It's the size of the market built around fixing billing performance. The global medical billing market was US$15.2 billion in 2023, rose to US$16.8 billion in 2024, and is projected to reach US$27.7 billion by 2029 at a 10.5% CAGR, according to MarketsandMarkets' medical billing market analysis.
That kind of growth tells you something important. Medical billing services are no longer a clerical afterthought. They sit much closer to treasury management than most practices admit. When billing works, cash arrives predictably, payer friction stays manageable, and leadership can plan. When it doesn't, the practice starts financing its own mistakes through delays, write-offs, and avoidable rework.
Too many leadership teams still frame the decision as a narrow debate about headcount. Keep billing in-house or outsource it. That's incomplete. The key question is how you govern reimbursement risk, how you measure operational discipline, and how you hold the billing function accountable for financial outcomes.
Table of Contents
- Why Medical Billing Is Now a C-Suite Conversation
- The Complete Revenue Cycle Management Workflow
- Deconstructing Medical Billing Service Offerings
- Measuring Success Key Performance Indicators
- In-House Versus Outsourced Billing A Strategic Analysis
- Your Vendor Selection and Implementation Roadmap
- Calculating the ROI of a Strategic Billing Partner
Why Medical Billing Is Now a C-Suite Conversation
A single weak billing process can slow cash, raise write-offs, increase compliance exposure, and frustrate patients at the same time. That is why medical billing now belongs in executive review, not just business office management.
The market shift supports that view. North America remains the largest regional segment for medical billing services, and earlier research cited in this article projects continued growth through 2029. The significance is straightforward. Providers are putting more of their financial performance behind specialized billing, coding, claims management, and denial recovery functions.
The cost of treating billing like clerical work
Billing should be managed like treasury operations with clinical inputs, not like routine paperwork. A practice can see steady patient volume and still miss budget if claims sit in edits, denials are not worked to root cause, or payment posting lacks discipline. I have seen organizations spend months negotiating supply costs while ignoring avoidable reimbursement leakage that had a larger impact on margin.
The problem is not just slower collections. Poor billing governance distorts forecasting, masks payer behavior, and leaves leaders reacting after cash misses the month.
A useful way to frame it is this: billing is where clinical documentation becomes cash, or fails to.
That is why executives need visibility into what happens between claim submission and payer decision. Teams that do not understand the claim adjudication process and its financial implications usually treat denials as an operations nuisance instead of a controllable source of margin loss and balance-sheet risk.
Practical rule: If leadership reviews staffing variance every month but reviews denial categories, underpayments, and aging trends only sporadically, it is monitoring the smaller risk.
What executives should actually ask
The right discussion starts with financial control, not vendor price.
- How predictable are collections? Can finance project cash with confidence, or does A/R timing move around because claims are aging unpredictably?
- Where does revenue break down first? Is rework driven by registration errors, eligibility gaps, coding issues, missing authorization, payer edits, or weak follow-up discipline?
- Who owns end-to-end performance? One leader or one partner should be accountable for clean claim rate, posting accuracy, denial recovery, and reporting quality.
- How quickly are problems escalated? When payer rules change or one service line slips, leadership should know who identifies it, how it is quantified, and how fast corrective action starts.
- What is the economic trade-off? A lower fee means little if it comes with slower cash, weaker controls, or poor visibility into write-offs and underpayments.
Medical billing services earn executive attention when they improve forecast accuracy, reduce preventable revenue loss, and give leadership evidence for decisions on staffing, payer strategy, and growth. That is a C-suite issue.
The Complete Revenue Cycle Management Workflow
Think of RCM as a financial circulatory system
A practice's revenue cycle management process works like a financial circulatory system. Registration is the intake valve. Coding turns clinical activity into billable data. Claims transmission moves the claim into the payer stream. Payment posting and denial management bring money back into the organization. If one point constricts, the whole system feels it downstream.
The visual below shows the full path in one view.
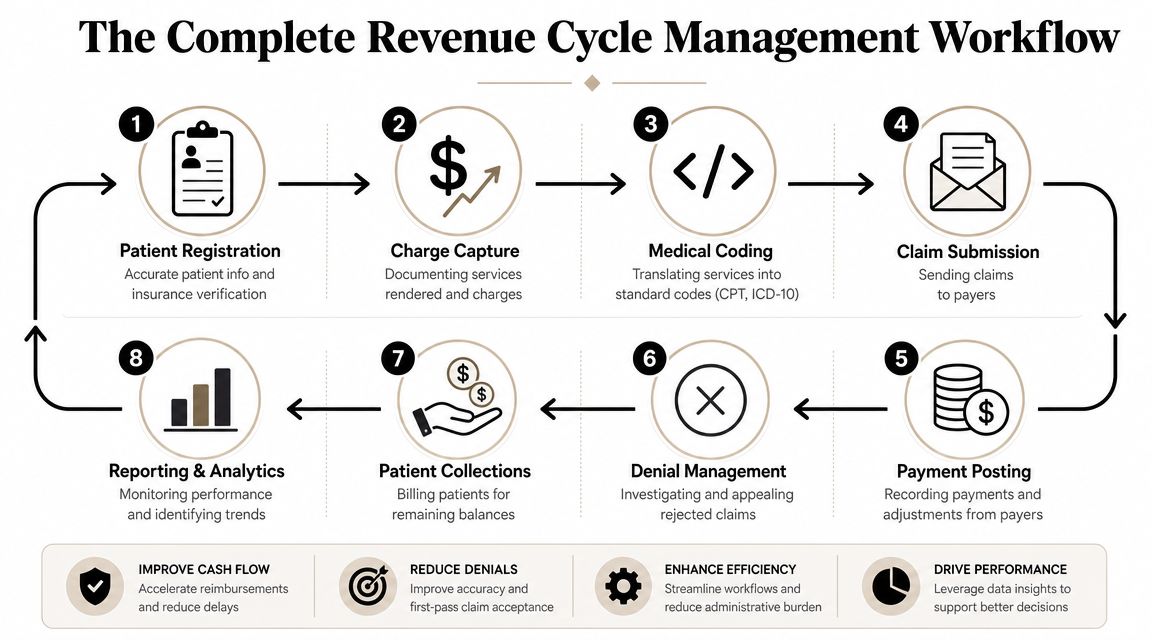
At the front end, patient registration and insurance capture have one job. Create a claim that can survive contact with payer rules. That means accurate demographics, current coverage, correct ordering or referring details when required, and complete authorization or referral support where applicable.
Eligibility work is especially impactful. Tight front-end verification matters because the average allowed amount per Medicare fee-for-service claim is only about $171, as noted by Expert Medical Billing Services on eligibility and benefits verification. In a high-volume practice, one preventable coverage miss doesn't just create a denial. It can erase the economics of the encounter once staff time and rework are added.
Where breakdowns become expensive
A clean workflow usually follows this sequence:
Pre-registration and intake
Staff confirm patient identity, payer details, and financial responsibility before the visit whenever possible.Eligibility and benefits verification
Teams confirm active coverage, plan limitations, coordination of benefits, and any authorization requirements.Charge capture and coding
Clinicians document what happened. Coders or billing staff translate that documentation into standardized codes and modifiers.Claim creation and submission
The practice prepares the claim file, scrubs it for edits, and sends it for payer processing and claim adjudication.Payment posting and reconciliation
Remittances are posted correctly, adjustments are reviewed, and mismatches get flagged instead of quietly accepted.Denial management and follow-up
Denials are worked by root cause, not just touched and closed.Patient billing and collections
After payer adjudication, the patient balance moves into a clear, timely collection workflow.Reporting and analytics
Leadership needs trend reporting that ties operational activity to cash results.
A denial usually starts long before the payer rejects the claim. Most of the time, the payer is only documenting a mistake the practice already made upstream.
A useful way to think about RCM is that every stage either preserves optionality or destroys it. If registration is weak, coders inherit missing data. If coding is late or inconsistent, claims miss filing windows or trigger edits. If payment posting is superficial, underpayments and denial patterns stay hidden. The workflow is sequential, but the financial consequences compound.
Here's where operators usually get it wrong:
| Workflow point | What works | What fails |
|---|---|---|
| Front end | Real-time eligibility checks and benefit confirmation | Treating insurance cards as proof of coverage |
| Coding | Specialty-aware documentation review | Coding from habit instead of current payer logic |
| Claim submission | Edit scrubbing before transmission | Measuring volume sent instead of clean claims accepted |
| Payment posting | Reconciliation and exception review | Posting cash without investigating variances |
| Denials | Root-cause tracking and timely resubmission | Working denials as isolated events |
| Patient billing | Clear statements and handoffs | Delayed, confusing patient balance workflows |
When leaders ask for “better billing,” this is what they should mean. Not more activity. Better control over every handoff that determines whether earned revenue becomes collected revenue.
Deconstructing Medical Billing Service Offerings
A billing contract that looks inexpensive on paper can still drain margin if the scope stops at claim submission. What practices are really buying is a control system for cash realization, compliance exposure, and reporting accuracy.
That distinction matters at the CFO level. Two vendors can quote the same percentage of collections and deliver very different financial results based on who owns eligibility, coding edits, payment variance review, denial appeals, and fee schedule maintenance.
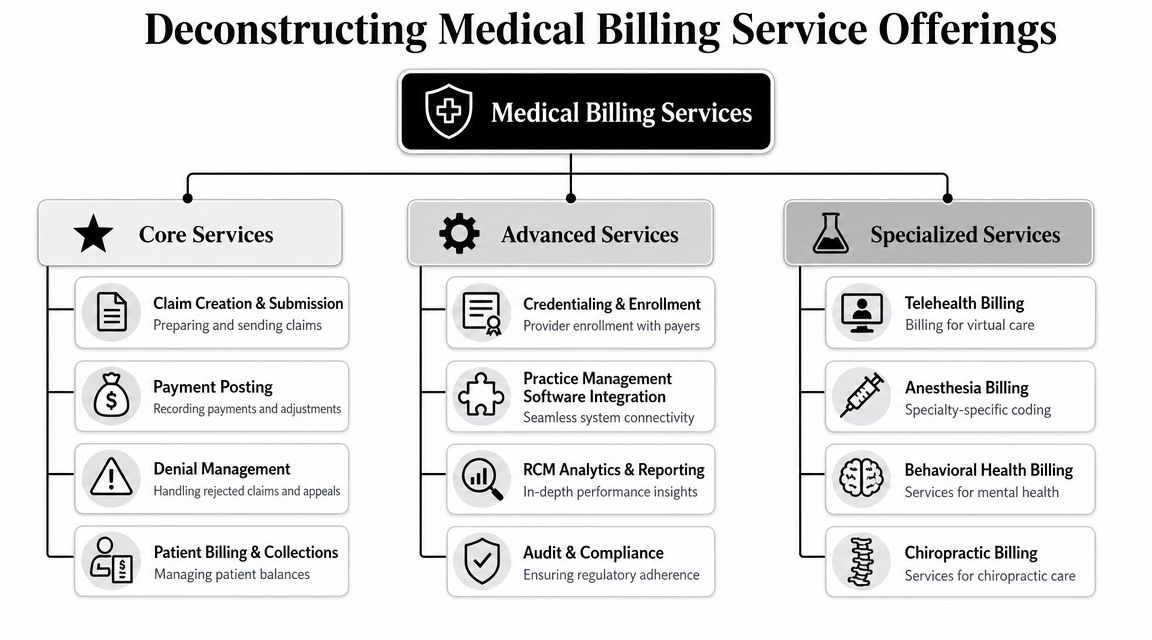
Core services that protect cash flow
The baseline service set should cover the functions that determine whether earned revenue turns into collectible cash.
- Insurance benefit verification checks active coverage, patient responsibility, and plan rules before the visit. Done well, it reduces avoidable denials and lowers the volume of patient balances that should have been identified upfront.
- Charge entry and claim creation translate documentation into a billable claim. Accuracy here depends on code selection, modifiers, units, place of service, and payer-specific edits lining up correctly.
- Claim submission and follow-up keep claims from stalling after transmission. Strong teams monitor clearinghouse rejections, payer acknowledgments, and unresolved claim statuses instead of measuring success by volume sent.
- Payment posting records payments and adjustments correctly, then flags variances that need review. If posting is treated as clerical data entry, underpayments and mapping errors stay buried in the ledger.
- Denial management sorts denials by root cause, payer, recoverability, and aging. That approach protects staff time and improves recovery rates because the team works the claims that still have economic value.
- Patient billing and collections support turn residual balances into statements and outreach patients can act on. Clear balance communication matters more now that patient responsibility represents a larger share of revenue for many practices.
Two often-overlooked functions sit underneath all of this. Fee schedule setup and practice management configuration determine whether claims and reports are built on sound logic or on manual workarounds. If the payer tables are wrong, even a disciplined billing team spends its time correcting system defects one account at a time.
Advanced and specialty support
After the core engine is stable, the next layer is about governance and performance management.
Some vendors include credentialing and payer enrollment, which can prevent revenue delays tied to provider setup, effective dates, and participation gaps. Others add RCM analytics, audit support, and custom work queues that help leaders spot deterioration earlier. For example, a vendor that can tie denial trends to underpayments and then connect both to your net collection rate performance gives finance leadership a more useful view than a basic aging report.
Workflow integration is another decision point with real operating consequences. The issue is not whether a vendor says it can work with your EHR or PM system. The issue is whether its process fits your environment without creating duplicate entry, offline trackers, or gaps between billing activity and financial reporting.
Service models also differ at this stage. Some organizations need a full outsourced partner with end-to-end accountability. Others need targeted support for front-end verification, denial recovery, payment posting, legacy A/R, or fee schedule cleanup. Clarity, for example, offers full-cycle and a la carte revenue cycle support, including fee schedule setup, insurance benefit verification, and payment posting.
The embedded overview below is useful if you want a quick visual summary before comparing vendors.
Buyers get into trouble when they purchase “billing” as a generic service. A better approach is to define which tasks the vendor owns, which tasks stay with internal staff, and how exceptions, variances, and missed deadlines are escalated.
A practical evaluation method is to map each service line to the financial or operational failure it is meant to prevent:
| Service offering | Problem it solves |
|---|---|
| Fee schedule setup | Underbilling, inconsistent charge logic |
| PM system configuration | Manual workarounds and reporting gaps |
| Eligibility verification | Coverage denials and patient balance confusion |
| Coding support | Incorrect code selection and modifier errors |
| Claim follow-up | Aging claims that stall after submission |
| Payment posting | Unreliable reporting and missed variance review |
| A/R management | Old balances that sit without triage |
| Compliance and audit review | Documentation and billing process risk |
That framing gives practice owners and finance leaders a better way to compare vendors. The purchase decision is not about “billing” in the abstract. It is about buying claim accuracy, posting integrity, denial recovery, payer accountability, and cleaner financial signal for management.
Measuring Success Key Performance Indicators
A practice can post charges accurately, submit claims on time, and still underperform financially if leadership tracks the wrong measures. KPI design is a governance issue, not a reporting preference. The job of a billing dashboard is to show whether expected reimbursement is converting into cash, where friction is building, and who owns the correction.
The visual below shows common target ranges. Use them as reference points, then adjust for specialty, payer mix, visit type, and the age profile of your current A/R.
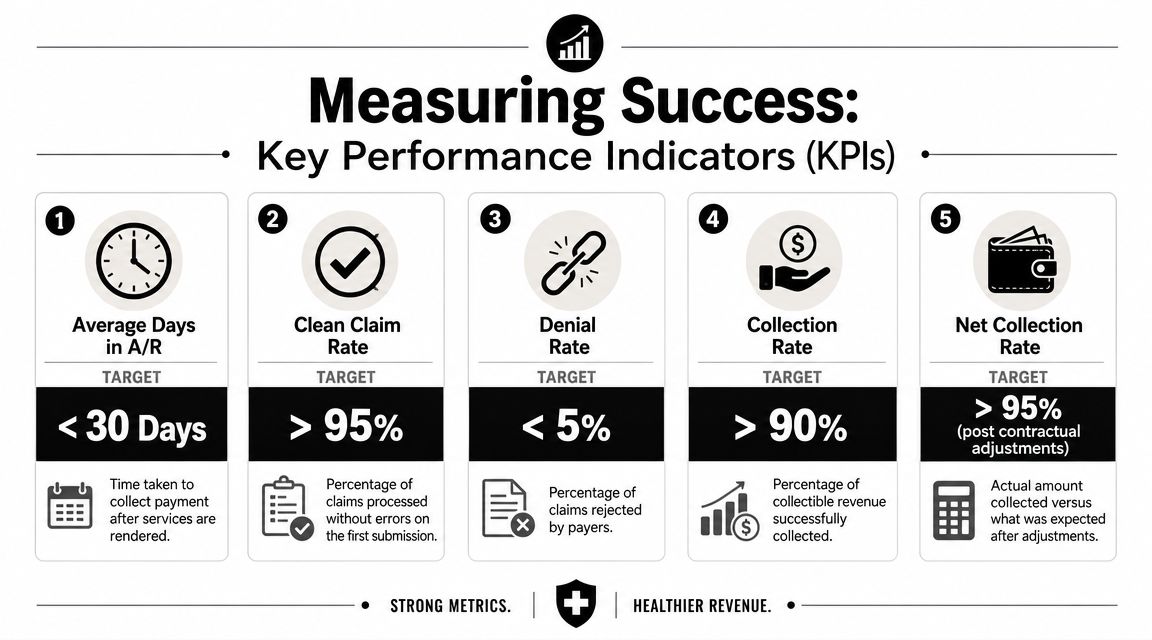
The KPI set that matters most
An executive team does not need twenty billing metrics. It needs a short set that ties operational performance to cash realization and forecast reliability.
| KPI | What it tells you | Simple formula |
|---|---|---|
| Net collection rate | How much collectible revenue you actually collect after contractual adjustments | Payments received ÷ adjusted charges |
| Days in A/R | How quickly the practice turns claims into cash | Ending A/R ÷ average daily charges |
| Clean claim rate | How many claims pass through correctly on first submission | Clean claims ÷ total claims submitted |
| Denial rate | How often payers reject claims | Denied claims ÷ total claims submitted |
| Gross collection rate | How much of billed charges the practice collects before adjustment logic | Total collections ÷ gross charges |
Of these, net collection rate usually deserves the most attention at the CFO and owner level because it strips out contractual noise and focuses on collectability. For a more detailed framework, this guide to net collection rate in healthcare RCM is a useful reference.
Gross collection rate still has value, but it is easy to misread. A strong gross rate can mask weak contract setup, write-off discipline, or payer underpayments. Net collection rate gives a cleaner view of execution.
How leaders should use these metrics
Each KPI should answer a management question.
- Use denial rate as a root-cause signal: Review denials by authorization, eligibility, coding, filing deadline, registration, and payer edit category. A single blended denial percentage hides the true failure point.
- Use days in A/R as a cash-flow signal: Rising A/R days can come from slow charge entry, delayed claim submission, weak follow-up, unresolved secondary claims, or payer behavior. The fix depends on where the queue is aging.
- Use clean claim rate as an early warning signal: This metric catches breakdowns before they spread into denials and older receivables. If first-pass quality drops, cash usually softens a few weeks later.
- Use net collection rate as the financial performance signal: It answers the question that matters most to ownership. Are we collecting what contracts and documentation support?
A useful billing report also assigns accountability. If a metric moved, the report should show the driver, the owner, and the expected date for correction. Anything less is activity reporting dressed up as management reporting.
Definitions matter just as much as results. I often see practices compare vendor reports against internal reports without confirming adjustment logic, legacy A/R treatment, refund handling, or whether small balance write-offs are included. That creates false confidence or false alarm. If the denominator changes, the trend loses meaning.
The strongest organizations treat KPI review the way a clinical team treats patient vitals. One bad reading may be noise. A sustained pattern usually points to an operational defect, a payer issue, or a control problem that is already affecting revenue.
In-House Versus Outsourced Billing A Strategic Analysis
The in-house versus outsourced decision is usually framed too narrowly. Practices compare a vendor fee to staff payroll and stop there. That misses the bigger issue, which is operating model design. You're deciding how to buy expertise, how to manage control, and where to place performance risk.
What in-house billing really buys you
An internal team gives leadership proximity. You can walk down the hall, review work queues directly, and shape workflow in real time. For some organizations, especially those with unusual provider schedules or complex internal politics, that access matters.
It also gives you tighter cultural integration. Front desk staff, coders, billers, and clinicians can solve issues quickly when everyone shares the same environment and the same daily cadence.
But in-house billing also creates fixed obligations. The U.S. Bureau of Labor Statistics notes that medical records specialists typically need a postsecondary certificate, and the median annual wage for the occupation was $50,250 in May 2024, with projected employment growth of 7% from 2024 to 2034 and about 14,200 openings per year, as summarized in Expert Billing Services' discussion of medical records specialist labor dynamics. For a practice owner, that signals a real labor market constraint. Skilled billing and coding talent isn't interchangeable administrative labor.
What outsourcing changes
Outsourcing converts part of the billing function from fixed staffing into a managed service relationship. That can improve flexibility, especially if volumes fluctuate, physician rosters change, or leadership wants broader specialty coverage without building multiple internal experts.
It can also improve discipline if the vendor has stronger standard operating procedures than the practice currently has. That's a big if. Outsourcing weak processes doesn't fix them. It just changes where they sit.
The main trade-off is governance. A vendor can perform well only if responsibilities are explicit. Who handles front-end registration quality. Who obtains authorizations. Who works denials by root cause. Who owns payer escalations. Who signs off on write-offs. If those lines blur, outsourced billing creates finger-pointing instead of control.
If your internal team is overwhelmed, outsourcing can help. If your governance is weak, outsourcing can make the weakness less visible but more expensive.
One useful reference point for evaluating team structure is the role definition itself. A strong billing operation needs analyst-level thinking around claim edits, denial trends, and payer patterns, not just transaction processing. That's why it helps to understand what a medical claims analyst does in RCM operations.
A practical comparison
Here's the side-by-side view CFOs usually need:
| Decision factor | In-house billing | Outsourced billing |
|---|---|---|
| Cost structure | More fixed payroll and training obligations | More variable service-based cost |
| Control | Direct oversight of staff and workflow | Indirect control through contract and reporting |
| Scalability | Slower to add specialty expertise or extra capacity | Easier to add coverage if vendor has bandwidth |
| Technology burden | Practice owns more setup, maintenance, and workflow design | Vendor may reduce internal administrative load, depending on model |
| Talent risk | Turnover hits operations immediately | Vendor absorbs some staffing volatility |
| Transparency risk | Problems are visible sooner | Problems can hide if reporting is weak |
| Compliance exposure | Internal training burden stays with the practice | Shared risk, but not transferred responsibility |
What works best often depends on stage.
- Smaller or growing groups often benefit from outsourced support because the alternative is building specialized capability before volume can justify it.
- Large groups with mature infrastructure may prefer internal control, especially when they already have strong management reporting and experienced supervisors.
- Hybrid models are often underrated. Some practices keep front-end intake and patient financial communication internal, then outsource coding, claims follow-up, denial work, or payment posting.
The wrong decision usually isn't in-house or outsourced by itself. The wrong decision is choosing a model that doesn't match your management capacity. If leadership won't review metrics, enforce workflow standards, and escalate payer issues, no structure will save the economics.
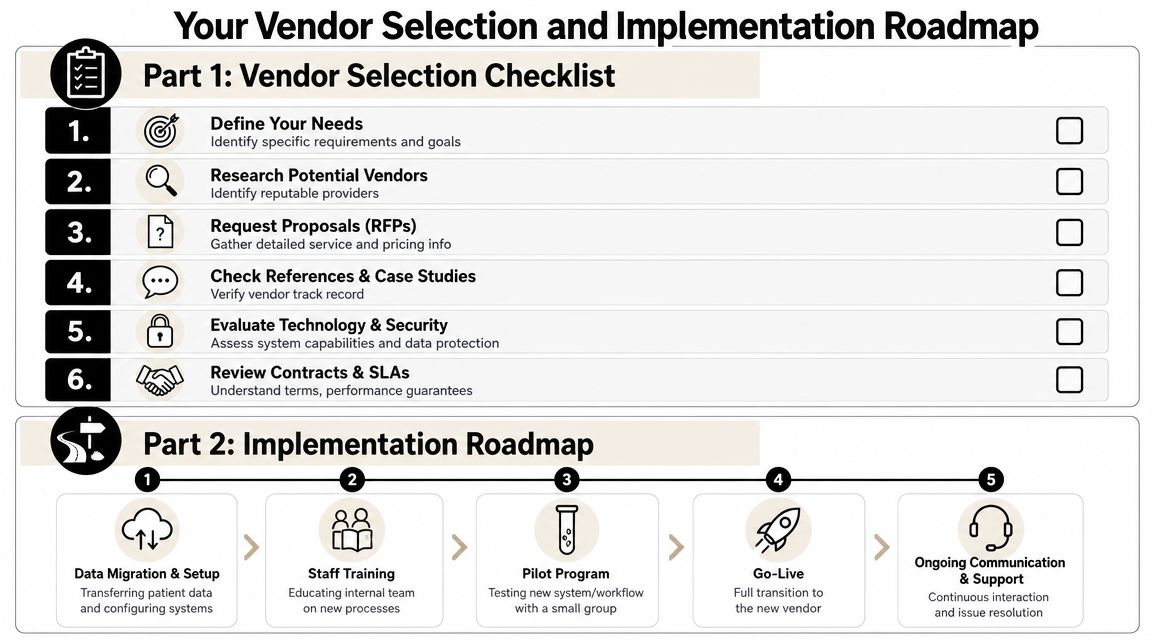
Your Vendor Selection and Implementation Roadmap
The medical billing vendor market is mature, fragmented, and full of similar claims. IBISWorld describes the U.S. medical billing services market as highly fragmented and notes a projected contraction in 2024, which is a useful reminder that buyers should focus less on “easy win” promises and more on governance and operating discipline, as reflected in IBISWorld's medical billing services industry analysis.
That changes how vendor selection should work. Don't shop for polished demos. Shop for evidence that the vendor can run a reliable operating system around your revenue cycle.
What to test before you sign
A solid vendor review should sound more like diligence for a financial partner than a software demo.
Use questions like these:
Scope ownership
Which tasks are fully owned by the vendor, which require your staff, and where are the shared handoffs?Reporting discipline
What reports arrive on what cadence. Can the vendor show denial trends, aging movement, payment posting accuracy, and work queue status in a format finance can use?Escalation structure
If performance slips, who on their side owns the account. Is there a named manager. How are payer escalations handled.System fluency
Can they work effectively in your existing EHR and practice management setup without heavy dependence on offline files and manual trackers?Controls and compliance
How do they document write-offs, adjustments, appeal activity, and access controls? Ask how exceptions are reviewed, not just how routine tasks are performed.Specialty fit
Do they understand the documentation and coding behaviors that drive denials in your specialty, or are they trying to apply a generic process everywhere?
Ask a vendor to show a sample monthly operating review. If they can't show you how they manage a client account in practice, don't assume the process exists behind the scenes.
A useful checkpoint is to request examples of how they handle bad inputs from the client. Real-life billing operations fail because information arrives late, incomplete, or wrong. A credible partner has a documented method for exception management.
What a disciplined implementation looks like
Implementation should be run like an operational transition, not a sales handoff. The sequence matters.
Discovery and baseline review
Confirm current payer mix, charge workflows, provider setup, outstanding A/R, denial categories, and system configuration.Data migration and configuration
Move payer tables, fee schedules, provider data, patient balances, and workflow rules carefully. Hidden configuration errors often surface during this stage.Workflow mapping
Define handoffs for registration, eligibility, coding, claim submission, payment posting, denial ownership, and patient balance communication.Training and communication
Front desk teams, clinicians, billers, and finance staff need role-specific instructions. Generic kickoff calls don't prevent workflow drift.Pilot or phased launch
Start with a manageable slice if possible. One location, one provider group, or one work queue can reveal process gaps before full rollout.Go-live with hypercare
Early days should include daily issue review, fast escalation, and close monitoring of edits, hold claims, and posting delays.Stabilization and monthly operating review
Once transaction flow normalizes, governance matters more than heroics. The vendor should deliver trend reporting, exception analysis, and a running list of corrective actions.
What fails in implementation is usually predictable:
| Implementation mistake | Likely result |
|---|---|
| Unclear ownership between practice and vendor | Denials bounce between teams |
| Weak data cleanup before migration | Old configuration errors continue into the new model |
| No baseline metrics before go-live | Nobody can prove whether results improved |
| Minimal front-desk training | Eligibility and registration errors keep feeding denials |
| No escalation cadence | Small issues sit until cash impact becomes obvious |
Vendor selection should end with a governance calendar, not just a signed agreement. If the first ninety days don't have named owners, reporting dates, issue logs, and decision rights, the practice is relying on hope.
Calculating the ROI of a Strategic Billing Partner
A CFO doesn't need a motivational argument for medical billing services. They need an ROI model. That model should connect billing performance to cash timing, collectability, labor burden, and management attention.
A finance-first ROI model
Start with four questions.
- What revenue is currently collectible but not collected
- How much staff time goes into avoidable rework
- How long does cash sit in A/R before resolution
- How much executive time gets consumed by billing exceptions
That gives you a practical framework:
| ROI component | Financial effect |
|---|---|
| Higher clean-claim performance | Less rework and faster first-pass payment |
| Better denial recovery | More earned revenue converted into cash |
| Tighter posting and reconciliation | Fewer unnoticed variances and cleaner reporting |
| Faster A/R movement | Better cash predictability and less balance aging |
| Lower internal management burden | More time for leadership to focus on growth and operations |
Use before-and-after measurement, but keep it simple. Compare the billing model on trend quality, reporting reliability, denial root-cause visibility, staff workload, and cash consistency. If a partner improves those areas, the economic value will usually show up through fewer preventable errors, better follow-up, and cleaner collections.
What good ROI usually looks like operationally
Consider a five-physician specialty practice evaluating whether to keep a strained internal billing team or move to a structured partner model. Don't force a fake benchmark. Instead, evaluate the transition through observable operating changes:
- Claims leave the system with fewer preventable edits.
- Eligibility failures get caught before the visit instead of after denial.
- Payment posting becomes reliable enough that finance trusts month-end reports.
- Denials are categorized, assigned, and worked to resolution instead of aging in a general bucket.
- Leadership receives a standard monthly operating review with actions, not just balances.
Those changes are easy to dismiss because they sound procedural. They aren't. They're the operating conditions that let a practice collect what it already earned.
I've seen leadership teams chase the wrong savings target here. They negotiate aggressively on billing fees while accepting weak reporting, vague accountability, and inconsistent follow-up. That can reduce visible expense while increasing hidden leakage. A cheaper billing function that misses collectible revenue isn't more efficient. It's just less transparent.
The better ROI question is this: does the billing model increase confidence in cash conversion? If the answer is yes, it's affecting enterprise value, not just office administration.
A disciplined billing partner should be able to help a practice do three things at once. Protect front-end accuracy, shorten the path from claim to cash, and give finance a reporting structure that supports decisions. When those three line up, the return isn't theoretical. It shows up in fewer surprises and better control.
If you're evaluating medical billing services through a CFO lens, Clarity is one option to review. The company provides full-service and a la carte healthcare revenue cycle support, including fee schedule setup, insurance benefit verification, billing operations support, claim status work, and payment posting. A practical next step is a consultation that maps your current workflow, identifies ownership gaps, and determines whether your biggest issue is front-end discipline, denial management, posting accuracy, or overall RCM governance.
No responses yet