Medical coding errors can drain millions from a hospital before the loss shows up clearly on a finance report. Reviewers and consultants routinely tie coding inaccuracy to material revenue loss, slower cash conversion, avoidable denials, and chart data that no longer supports the care that was delivered.
For a CFO, this sits inside revenue integrity, not just HIM or the business office. A coding miss does more than reduce a claim. It can trigger rebilling work, appeal labor, audit exposure, and bad downstream reporting for service line performance, payer behavior, and physician documentation trends.
The operational drag usually starts upstream. Weak documentation, inconsistent charge entry, and gaps in charge capture workflows often feed the coding queue with incomplete or conflicting information. Coding then works like a translation layer between the clinical record and the claim. If the source language is sloppy, the financial output will be wrong.
The organizations that manage this well do not stop at asking which codes are wrong. They rank coding risk by financial exposure, denial volume, compliance sensitivity, and rework burden, then audit where one error causes five more problems later in the revenue cycle.
Table of Contents
- The Hidden Cost of Medical Coding Errors
- A Taxonomy of Common Medical Coding Errors
- Quantifying the Full Impact on Your Organization
- How to Detect and Audit Coding Inaccuracies
- A Practical Framework for Error Mitigation
- Plugging Revenue Gaps with an RCM Partner
- An Executive Checklist for Coding Accuracy
The Hidden Cost of Medical Coding Errors
Industry estimates often put revenue loss from inaccurate or incomplete coding in the low single digits. For a hospital with $500 million in annual net patient revenue, even a 1% miss is a $5 million margin problem. That is why coding accuracy belongs in the finance conversation, not just the HIM queue.
The cost extends beyond a single denied or underpaid claim. A coding error can trigger rework across utilization review, billing edits, claim status follow-up, patient statements, appeal handling, and audit response. What looks small at the claim level becomes expensive at scale because each exception pulls labor out of teams that should be closing clean accounts.
Revenue leakage usually starts upstream. In many organizations, the denial shows up at the back end, but the defect began earlier with incomplete documentation, missed charges, or code selection that did not reflect the encounter with enough specificity. The handoff between clinical care and reimbursement is where cash is either preserved or lost, especially in processes tied to charge capture accuracy and workflow design.
I tell CFOs to separate direct loss from operational drag. Direct loss includes undercoding, delayed payment, avoidable write-offs, and missed appeal windows. Operational drag is the hidden tax: coder queries, rebills, edit workqueues, payer calls, compliance reviews, and staff overtime. Both matter. One hits revenue. The other raises cost to collect.
Coding also carries uneven risk. A minor registration typo may slow a claim. A pattern of modifier misuse, unsupported E/M levels, or missed diagnosis specificity can affect reimbursement, case mix, compliance exposure, and quality reporting at the same time. The right response is not to audit everything equally. It is to rank error types by financial impact, audit exposure, and recurrence, then put resources where the loss is largest.
From a CFO seat, coding is the translation layer between clinical work, contractual reimbursement, and defensible reporting. If that translation is weak, the organization pays twice. First in missed or delayed cash, then in the labor required to clean up preventable errors.
A Taxonomy of Common Medical Coding Errors
The easiest way to understand medical coding errors is to think of a mailroom. If the envelope has the wrong address, the wrong contents, or the right contents with the wrong label, it doesn't reach the right destination cleanly. Claims work the same way.
Some errors are obvious. Others are subtle enough to pass internally but still fail payer logic. The most expensive ones usually involve code combinations, modifiers, specificity, sequencing, and documentation support.
Why these mistakes keep happening
Bundling logic is a common trap because the rules aren't intuitive. The AMA notes that unbundling happens when component services are billed separately instead of using the single code that represents the full procedure. It also warns that incorrect modifier use can invalidate a claim, including cases such as using modifier 50 when the code already includes bilateral service or overusing modifier 22 without documentation (AMA guidance on coding mistakes that cost practices money).
That's why coding teams can't rely on memory, old cheat sheets, or habit. Payers compare code combinations against procedure rules. If your logic doesn't match theirs, the claim can fail even when the underlying care was medically necessary.
A practical analogy helps here. Unbundling is like a restaurant charging separately for the bun, patty, cheese, and lettuce when the menu item is a burger. You may have served all the components, but the pricing logic is wrong.
Common medical coding error categories
| Error Category | Description | Example |
|---|---|---|
| Specificity errors | The code is too vague for the documentation and payer requirements | Choosing a less specific diagnosis when the chart supports a more precise one |
| Sequencing errors | Codes are listed in an order that doesn't reflect the principal reason for the encounter | A secondary condition placed where the primary condition should be |
| Bundling errors | Separate components are billed instead of the comprehensive procedure code | Billing parts of a procedure individually rather than the single inclusive code |
| Modifier errors | A required modifier is missing, unsupported, or incorrectly applied | Modifier 50 added to a code that already includes bilateral service |
| Documentation mismatch | The record doesn't support the submitted diagnosis or procedure code | A higher-acuity service level submitted without documentation to justify it |
| Code currency errors | The code set used doesn't reflect current requirements | A team continues using an outdated code after annual updates |
| Duplicate billing errors | The same service is submitted more than once | A repeated charge enters the claim after handoff confusion |
Coding leaders should teach categories, not just isolated mistakes. Staff who understand the error family catch more issues than staff who memorize examples.
One more point matters for specialty groups and hospitals with mixed service lines. Behavioral health, surgery, emergency care, therapy, and hospital-based services all have different denial patterns. If your billing team is seeing recurring payer pushback in one specialty, it helps to compare that against known denial pressure points such as behavioral health CPT billing denials.
Quantifying the Full Impact on Your Organization
A coding error has at least four possible consequences. It can reduce revenue, consume labor, increase compliance exposure, and contaminate the clinical record. Most organizations measure the first one and underestimate the other three.
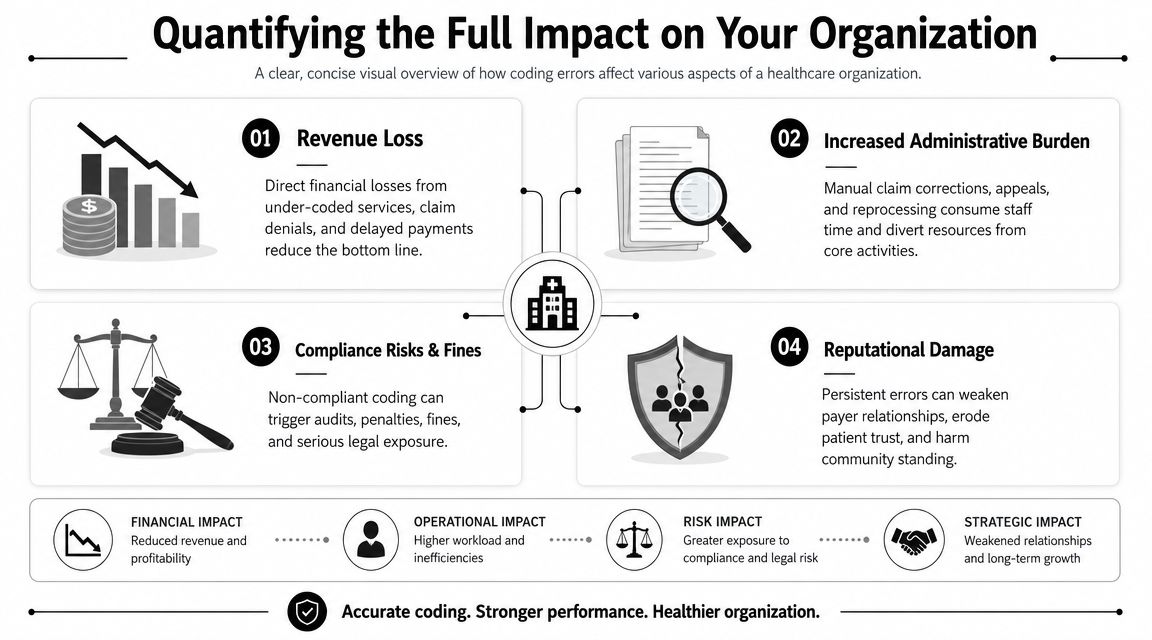
Financial and operational drag
Finance teams usually see the visible symptom first. Cash slows down, denials increase, and net revenue comes in below expectation. But the actual operational burden shows up in the rework queue. Staff have to retrieve charts, review documentation, correct codes, touch payer portals, resubmit claims, and answer follow-up questions. Every avoidable correction steals time from cleaner work.
That's why I advise CFOs to look beyond gross collections and monitor whether coding quality is undermining the organization's net collection rate performance. If the denominator looks healthy but the back-end team is doing constant cleanup, the revenue cycle is carrying hidden friction.
A useful executive test is simple:
- Check where work repeats: Which claims require multiple touches after submission?
- Check who is doing the rework: Are experienced billers spending time on preventable corrections?
- Check where cash stalls: Do certain service lines always need manual intervention before payment posts?
Compliance and clinical consequences
Compliance risk enters when coding choices can't be defended. Incorrect bundling, unsupported modifiers, and diagnosis-to-procedure mismatches can trigger payer scrutiny, recoupments, and external review. Even when the organization's intent was not improper billing, weak coding discipline creates a pattern auditors notice.
The clinical impact is often missed in financial discussions. Clinical coding errors can persist inside the structured record and affect future prescribing, triage priority, disease-register inclusion, and decision-support alerts. A 2024 systematic review of 25 studies found that coding errors can transmit misinformation through clinical decision-support systems and cause direct patient harm, with upstream drivers including poor documentation, clinician fatigue, and legacy template design that reduce coding completeness and specificity (systematic review summary on coding errors and patient safety).
A bad code doesn't just misstate the bill. In some cases, it changes what the next clinician sees as truth.
That's why medical coding errors belong on the executive risk agenda. They sit at the intersection of margin, labor efficiency, compliance, and patient safety.
How to Detect and Audit Coding Inaccuracies
Random audits have their place, but they don't give leadership enough control. If you sample charts without a risk model, you often find low-value mistakes while the expensive problems stay buried in specific specialties, providers, or workflows.
Recent guidance on coding updates points to a real gap in the market. Sources note that FY 2024 brought more specific and granular coding requirements and recommend ongoing audits, but they don't offer specialty-level risk ranking or benchmark data to tell leaders where to aim first (discussion of newer specificity requirements and the need for ongoing audits). That means each organization has to build its own prioritization logic.
Start with risk, not random sampling
A practical audit plan starts by asking where coding complexity meets financial exposure. In most hospitals, that means prioritizing areas with one or more of these characteristics:
- High denial recurrence: Service lines where the same coding-related denial reasons keep returning
- Frequent rule changes: Specialties affected by code-set updates, documentation specificity shifts, or payer nuance
- High documentation variability: Providers whose notes are clinically sound but structurally inconsistent for coding
- High-value encounters: Cases where a small coding miss creates outsized reimbursement or compliance consequences
Internal audits work best for routine surveillance. External reviews work best when leadership needs an independent read on accuracy, physician variation, or systemic process weaknesses.
Build a monitoring loop
The strongest teams don't audit once and move on. They create a feedback loop between coding, CDI, billing, compliance, and physician leadership. You want the audit output to answer operational questions, not just produce error counts.
Track patterns such as:
- Denial reason concentration: Which coding-related denial reasons dominate by payer and specialty?
- Provider variation: Which physicians generate the highest documentation query volume or coding corrections?
- Pre-bill edit trends: Which edits fire most often, and which ones still escape into denials?
- Rework burden: Which claim types repeatedly return for manual correction?
Audit for decision-making, not for shelfware. If the report doesn't change education, edits, or workflow ownership, it's paperwork.
A CFO doesn't need every coding detail. The CFO needs a ranked list of risk areas, a clear owner for each one, and a timetable for whether the intervention is working.
A Practical Framework for Error Mitigation
Analysts at Grand View Research estimate that the U.S. medical coding market will grow from $21.6 billion in 2025 to $44.4 billion by 2033, which tells CFOs something simple. Health systems keep spending here because coding errors are not a nuisance line item. They create measurable drag on cash, labor, compliance, and forecasting.
A practical mitigation plan starts by ranking risk, not by issuing broad reminders to "code more accurately." The goal is to reduce the errors that create the highest financial and operational cost first. A missing diagnosis detail on a low-dollar claim and a modifier error on a surgical case are both coding mistakes, but they do not carry the same reimbursement or audit exposure. Treating them the same wastes staff time.
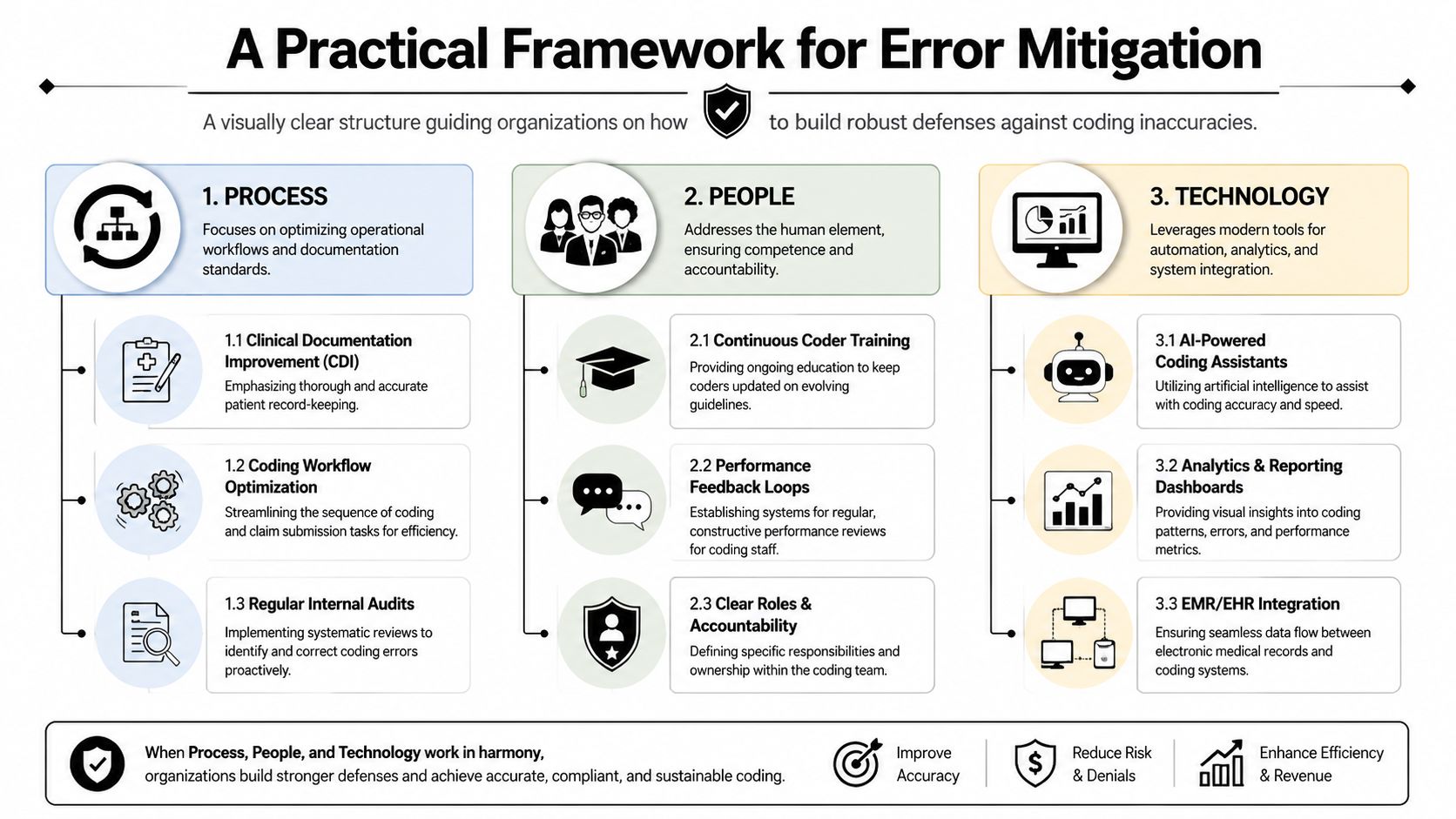
Process
Process is where preventable rework starts or stops.
If documentation arrives late, queries stall, or edits happen after submission, the organization has built a correction factory instead of a clean claim process. Every handoff adds delay. Every late fix pulls skilled staff into low-value rework.
Focus process improvement on three points:
- Clinical documentation improvement: Coders and CDI staff need defined escalation paths when specificity is missing or conflicting.
- Coding workflow design: Separate judgment-based coding review from routine data cleanup so certified coders spend time on cases that require interpretation.
- Pre-bill controls: Place edit logic before claim submission, where errors are cheaper to fix and less likely to turn into denials.
Strong process design works like quality control on a manufacturing line. Catch defects before the product ships. Do not build a department around returns.
People
Coding accuracy is also a management discipline. Teams need clear ownership, specialty-specific education, and feedback tied to recent error patterns.
Broad annual training rarely changes denial trends. Targeted coaching does. If orthopedic cases are losing revenue because modifiers are applied inconsistently, teach those exact scenarios. If inpatient coding quality depends on physician specificity, train providers and coders together on the documentation gaps driving DRG movement, queries, or payer pushback.
Accountability needs to be explicit:
- Coders own code selection quality
- Providers own documentation completeness
- Billing leaders own denial feedback and escalation
- Compliance owns policy alignment and audit response
Shared responsibility sounds collaborative, but in practice it often means no one closes the loop.
Technology
Technology should reduce variation, support judgment, and show leaders where risk is pooling. It should not become a substitute for coder review or operational discipline.
Computer-assisted coding, claim scrubbers, analytics dashboards, and EHR prompts can improve performance when they are tuned to actual workflows and payer rules. They fail when alerts are ignored, edit libraries are outdated, or coding and billing systems do not share the same logic. In that setup, leadership sees activity on a dashboard and assumes control exists. The denials say otherwise.
Some hospitals build the full stack internally. Others use a partner for targeted functions such as fee schedule setup, billing operations support, benefit verification, and claim status follow-up. Clarity's healthcare revenue cycle management services are one example of that targeted support model, used when leadership needs to close specific operating gaps without handing off the entire revenue cycle.
The practical standard is simple. Put the most experienced people on the highest-risk work, automate the repeatable checks, and measure whether each change reduces denials, rework, or revenue leakage within a defined timeframe. If it does not change one of those three outcomes, it is not mitigation. It is overhead.
Plugging Revenue Gaps with an RCM Partner
Some organizations have the internal depth to manage coding improvement on their own. Many don't. The challenge isn't just expertise. It's maintaining expertise while handling code changes, payer behavior, staffing turnover, denial follow-up, and daily claim volume.
When internal capacity isn't enough
The warning signs are usually operational, not theoretical. Coding quality varies by team. Denial trends are known but not acted on. Managers spend more time redistributing work than fixing root causes. Education becomes reactive. The business office keeps solving the same problem in slightly different forms.
In that environment, outside help can make sense because it gives leadership faster access to specialized workflows, cleaner accountability, and more consistent operating discipline.
An RCM partner is useful when the organization needs help with:
- Foundational setup: Fee schedules, practice management configuration, and cleaner billing rules
- Daily execution: Billing operations support across specific functions where internal teams are thin
- Front-end denial prevention: Insurance benefit verification and eligibility work before the claim ever drops
- Back-end cash recovery: Claim status review and payment posting to keep A/R moving accurately
What an external partner should actually fix
A partner shouldn't just absorb volume. The partner should help leadership remove recurring failure points. That means clearer work queues, tighter edits, stronger follow-up discipline, and better visibility into where revenue is leaking.
Video can help executive teams evaluate whether that operating model fits their environment:
The right decision comes down to control and speed. If your internal team can build reliable coding governance, keep pace with change, and hold denial rework down, keep it in-house. If not, a specialized RCM partner can close the gap without forcing leadership to rebuild the entire revenue cycle from scratch.
An Executive Checklist for Coding Accuracy
A coding program does not need perfect charts. It needs predictable control over where errors occur, how often they recur, and what they cost the organization.
For a CFO or revenue cycle leader, this checklist is less about coding theory and more about risk ranking. A missed modifier on a low-volume claim is not the same problem as repeated documentation gaps in a high-dollar service line. The first is noise. The second is margin erosion.
Use this checklist in your next revenue cycle review:
- Confirm documentation quality: Are CDI efforts improving record completeness in the departments, providers, and encounter types where coding errors create the largest financial exposure?
- Test coder education: Is training tied to payer edits, specialty-specific risk, and recent internal audit findings, or is it still broad and generic?
- Review audit coverage: Are audits aimed at your highest-risk services, denial-prone codes, and outlier providers, rather than relying on random samples alone?
- Inspect pre-bill controls: Do edits stop modifier, sequencing, and bundling errors before claims leave the door, or is staff fixing them after denials hit A/R?
- Measure rework burden: Can leadership quantify where billing and coding teams spend time correcting preventable errors, and what that labor is costing?
- Check cross-team accountability: Do coding, CDI, billing, compliance, and physician leadership each own specific corrective actions with deadlines and follow-up?
The strongest teams treat coding accuracy like air traffic control. Small misses matter, but the primary job is preventing the collisions that disrupt the whole system.
Medical coding errors are manageable when leadership treats them as an operating problem with measurable financial drag. That shift helps protect revenue, reduce avoidable rework, and focus audits where the return is highest.
If your organization needs an outside assessment of coding-related revenue leakage, Clarity offers a complimentary consultation to review the current revenue cycle and identify targeted opportunities to improve accuracy, efficiency, and margin.
No responses yet