Most advice about the medical claims analyst role is too small. It treats the job as claim cleanup, denial follow-up, and coding support. That framing misses where the core value sits.
A strong medical claims analyst doesn't just move claims through a queue. They protect margin, catch revenue leakage before it repeats, and translate payer behavior into operational fixes that leadership can use. For a CFO, CEO, or physician owner, that difference matters. The question isn't whether someone can work denials. The question is whether they can show you why those denials keep happening, which problems are worth fixing first, and how to stop preventable rework from draining cash flow.
Table of Contents
- Beyond Processing The Strategic Role of a Medical Claims Analyst
- A Day in the Life Core Workflows and Responsibilities
- Skills KPIs and Salary Benchmarks for Top Talent
- How to Hire an Effective Medical Claims Analyst
- The Executive Decision Hiring In-House vs Outsourcing to a Partner
- Secure Your Revenue Cycle with an Expert Partner
Beyond Processing The Strategic Role of a Medical Claims Analyst
The common mistake is calling the medical claims analyst a back-office processor. That's inaccurate, and it leads executives to underinvest in one of the most important control points in the revenue cycle.
A medical claims analyst is a specialized professional who reviews claims for accuracy, verifies diagnoses against payer rules, applies coding standards, and investigates discrepancies. The role has defined progression levels in Michigan's state specification, from entry through more advanced levels, which signals that employers have long treated it as an analytical, rule-driven function rather than clerical work. That same framework also places analysts in regulated payment environments such as workers' compensation, not just routine commercial claims workflows, as described in this overview of the medical claims analyst role and progression path.
Why the role is analytical, not clerical
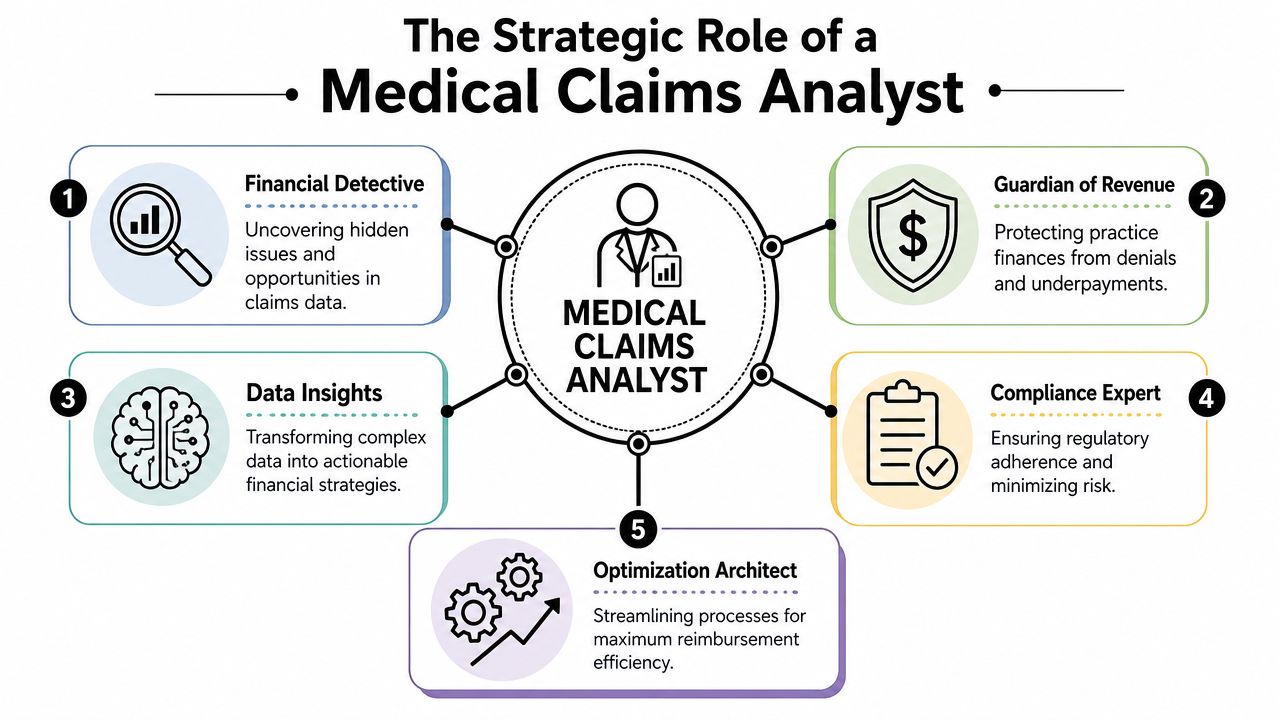
Think of the analyst as a financial detective inside your revenue cycle. Billing teams submit work. Coders translate documentation. But the analyst sits at the point where payment rules, documentation quality, contract logic, and operational defects all collide.
That's why the best analysts do more than ask, “Was this claim sent?” They ask:
- Was the claim build defensible under the payer's rules and the patient's benefits?
- Did the denial reveal a one-off error or a recurring system defect?
- Is this underpayment tied to contract terms, pricing logic, or configuration?
- Will the same issue hit the next hundred claims if nobody changes the process?
Practical rule: If your claims staff only fix individual denials, you're paying for rework. If they identify root causes and stop recurrence, you're building margin protection.
In this context, healthcare revenue cycle analytics becomes relevant. The role makes sense only when leadership sees claims as data, not just transactions. Every denial reason, edit failure, authorization miss, and underpayment pattern tells you something about front-end intake, coding consistency, payer setup, or internal workflow design.
Where executives feel the impact
Executives usually notice claims analysis only when cash slows down. That's late.
The earlier signal is operational friction. Staff spend too much time reopening claims. Appeals deadlines get missed. Payment posting uncovers mismatches that no one can explain. One payer suddenly behaves differently, and the organization doesn't know whether the issue sits in registration, coding, contract setup, or filing logic.
A strong analyst reduces that ambiguity. They connect claim errors to specific fixes, assign ownership, and turn payer noise into a usable management signal.
Here's what doesn't work. Hiring someone who can touch many claims per day but can't explain patterns. That person may keep the work queue moving, but they won't protect the practice from repeated leakage.
What works is hiring for judgment. A capable analyst can tell leadership whether a denial spike is a coding mismatch, an authorization workflow defect, a policy interpretation issue, or a system configuration problem. That's a different level of value entirely.
A Day in the Life Core Workflows and Responsibilities
The daily work of a medical claims analyst is methodical, but it isn't repetitive in the simplistic sense. The workflow blends payer rule interpretation, code validation, follow-up discipline, and pattern recognition. When that work is done well, reimbursement becomes cleaner and denials become more actionable.
A useful visual overview sits below.
How a capable analyst works a claim
At the technical level, the role centers on adjudicating claim validity. The analyst reconciles diagnosis and procedure codes, such as ICD-10 and CPT, against payer policies, benefits, and supporting documentation. They also correct and resubmit denied claims across Medicare, Medicaid, workers' compensation, and commercial lines, as outlined in this description of claim adjudication responsibilities for medical claims analysts.
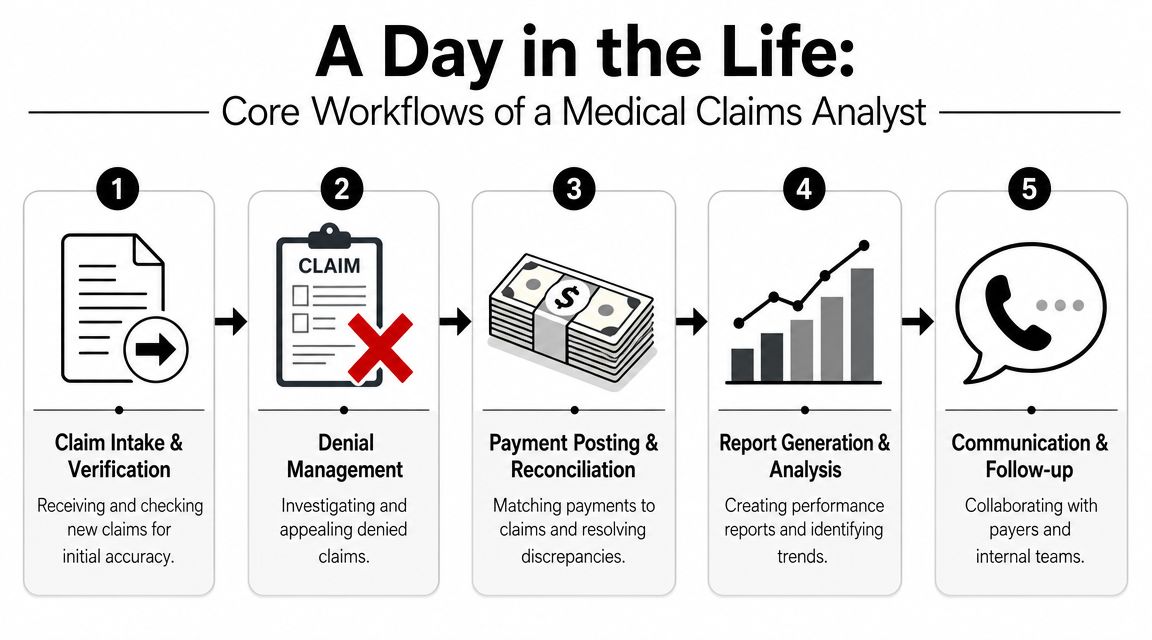
In practice, the day often moves through a sequence like this:
Intake review
New claims or denial worklists come in from the billing platform, clearinghouse, or payer portal. The analyst checks whether the record is complete enough to act on.Code and policy validation
Diagnosis and procedure coding must align with the documentation and the payer's benefit rules. Small mismatches create avoidable rework.Denial or discrepancy investigation
If the payer rejected, denied, or underpaid the claim, the analyst identifies the exact reason and traces it back to the source.Correction and resubmission
The analyst updates the claim, compiles support if needed, and resubmits within the required timeframe.Trend capture
The individual claim is done, but a proficient analyst logs the issue category so operations can see whether it's isolated or recurring.
For leaders who want a plain-language view of that process, this guide on what claim adjudication means in practice is a useful reference.
A quick explainer helps clarify the flow:
What good denial management looks like
The difference between average and strong performance shows up after the denial.
An average worker sees a denial and asks, “How do I fix this claim?” A strong analyst asks, “Why did this happen, who owns the root cause, and how do we stop it from hitting the next batch?”
Fixing a denied claim recovers one payment. Fixing the process that caused it protects future cash flow.
A practical example: a claim is denied because the procedure code doesn't align with the diagnosis documentation under the payer's edit rules. The weak response is to correct that one submission and move on. The stronger response is to check whether the issue came from template misuse, coding education gaps, or a payer-specific rule that hasn't been built into the team's pre-bill review.
That distinction is why executives shouldn't evaluate the role only on speed. Speed matters. But speed without reasoning just accelerates recurring mistakes.
Skills KPIs and Salary Benchmarks for Top Talent
Executives often hire this role too low in the org chart and then wonder why denials keep resurfacing. A strong medical claims analyst does more than clear work queues. This person finds where revenue leaks start, quantifies the impact, and gives operations a basis for fixing the source.
That distinction should shape how you define top talent.
The baseline is easy to find. Many candidates know coding rules, payer terminology, and common billing workflows. The harder question is whether they can trace underpayments, denials, and rework back to a repeatable operational problem and show what that problem is costing the practice. That is why the role now includes trend analysis, exception tracking, appeal management, and review of paid-versus-denied patterns across payers and service lines, as outlined in this professional claims analyst job description.
What skills separate strong analysts
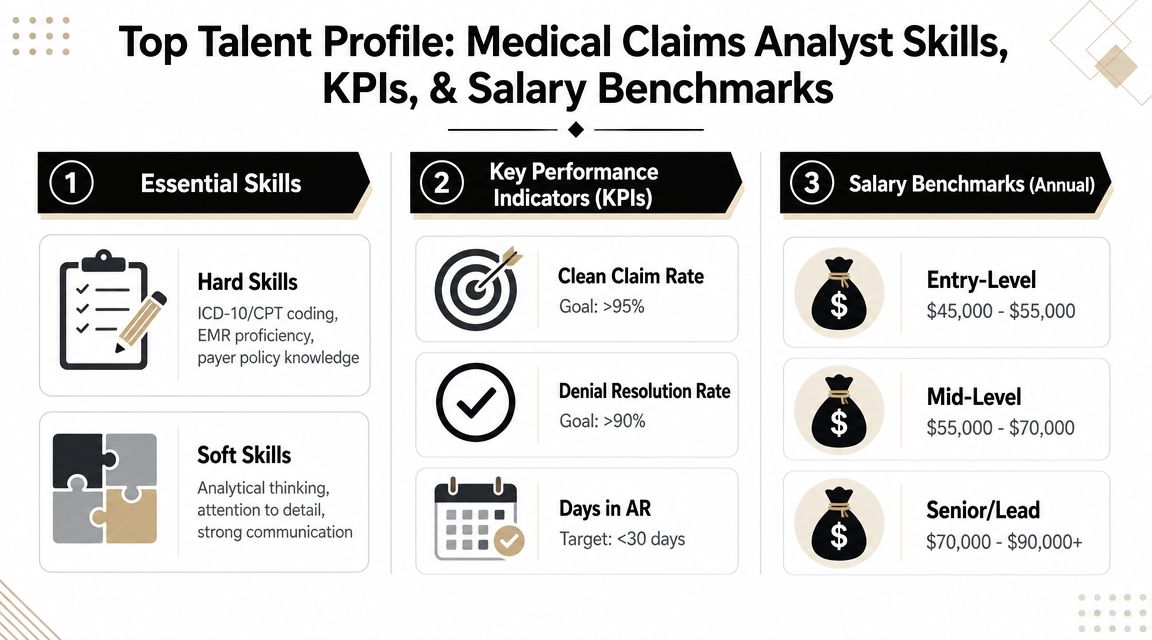
The best analysts combine technical fluency with financial judgment. They understand that every denial category has an owner, a cause, and a cash consequence.
| Skill area | What leadership should look for |
|---|---|
| Coding and documentation fluency | The candidate can spot where ICD-10, CPT, documentation, and payer edits conflict before the issue spreads |
| Payer rule interpretation | They understand that Medicare, Medicaid, workers' compensation, and commercial payers follow different rules, timelines, and edit logic |
| Systems fluency | They can work within billing systems, payer portals, work queues, and reporting tools without losing control of the handoff |
| Root-cause analysis | They ask what triggered the variance, how often it occurs, and which team needs to change its process |
| Communication | They can explain a denial pattern to coding, front desk, utilization review, and finance teams in plain language |
Attention to detail matters, but detail alone does not protect margin. The role also requires enough judgment to challenge a bad workflow, enough discipline to document findings clearly, and enough credibility to push corrective action across departments. In practice, that is what separates a processor from an operator who protects revenue.
Which KPIs leadership should watch
A useful dashboard for this role is short. It should show whether the analyst is reducing preventable loss, shortening recovery time, and identifying recurring defects before they hit cash.
Focus on measures like these:
Denial patterns by root cause
The analyst should be able to show whether recurring denials start in scheduling, eligibility, authorization, coding, charge entry, or payer setup.Paid versus denied mix by payer and service line
This helps leaders see whether a variance is isolated or tied to a broader workflow issue.Appeal timeliness and filing window performance
Good analysis has limited value if appeals miss payer deadlines and turn recoverable dollars into write-offs.Rework volume
High rework usually means the practice is correcting defects after submission instead of preventing them before claim drop.Recovery yield from corrected claims and appeals
This shows whether analyst effort is producing cash or just producing activity.
Leaders should also connect analyst performance to broader financial outcomes such as net collection rate performance across the revenue cycle. One analyst does not own that metric alone, but this role has direct influence on whether earned revenue becomes collected cash.
Watch for a common management mistake: measuring queue closure without measuring defect reduction. Fast closure can still leave the same denial category hitting next week's batch.
What the market says about compensation
Compensation should match the financial responsibility attached to the role. Employers hiring for medical claims analysts commonly assign work tied to claim review, discrepancy research, eligibility validation, denial investigation, and exception handling. In the current market, that work is paid accordingly, with hourly ranges that often sit above entry-level billing support because the job carries direct revenue risk and requires independent judgment.
The practical takeaway is simple. If you hire for low-cost task execution, you usually get low-cost task execution. If you hire for root-cause analysis, payer pattern recognition, and cross-functional problem solving, you improve collections, reduce avoidable rework, and protect future cash flow. That is usually the better bargain.
How to Hire an Effective Medical Claims Analyst
The hiring mistake is predictable. Leadership screens for claim exposure, software familiarity, and years in billing, then wonders why denials keep repeating and underpayments stay buried in aging.
A strong medical claims analyst protects margin by finding why revenue is leaking in the first place. The hire should be able to trace a denial pattern back to registration, authorization, coding edits, payer setup, or follow-up rules, then push the issue to the team that can stop it from recurring. That is different from filling a queue.
Earlier sections covered compensation and market signals. The practical hiring takeaway is simpler. Recruit for analytical judgment tied to cash impact, not just task familiarity.
A job description that attracts analysts, not processors
The job post should describe the business problem you need solved.
Use language like this:
We need a medical claims analyst who can review claims for accuracy, investigate denials and underpayments, identify recurring payer or workflow issues, support appeals, and turn claims findings into corrective actions for billing, coding, front-end, and management teams.
That framing changes the candidate pool. Experienced processors will still apply, but stronger applicants will recognize that the role carries ownership for defect reduction, not just claim movement.
A useful job description should set expectations in five areas:
Claim review ownership
The analyst checks coding, documentation alignment, payer rules, and claim completeness before small errors become payment delays or write-offs.Denial root-cause analysis
Resubmission is only one part of the work. The larger job is finding the operational source of repeated denials and documenting what needs to change.Trend reporting
The analyst should be able to summarize paid versus denied activity, underpayment patterns, and rework drivers in a way executives can act on.Cross-functional communication
Claims issues rarely stay inside the billing office. The role needs someone who can work with coders, front-desk staff, payment posting teams, and managers without losing the thread of the problem.System awareness
Good analysts work inside queues, payer portals, edits, reports, and issue logs. Spreadsheet skill helps, but it is not enough on its own.
One sentence in the posting matters more than leaders think: who owns follow-through. If the analyst only "reviews and reports," the role becomes passive. If the analyst is expected to identify issues, assign operational owners, and confirm resolution, you are hiring for revenue protection.
Interview questions that reveal problem solvers
Resumes rarely show this well. Interviews do.
Ask candidates to explain how they worked from symptom to cause, what evidence they used, who they involved, and what changed after the fix. If they cannot describe that chain clearly, they are unlikely to improve yield once hired.
Use questions like these:
- Tell me about a denial trend you found before anyone assigned it to you. What pointed you to the issue, and what changed after you addressed it?
- Describe a case where the first explanation was wrong. How did you determine the actual cause?
- How do you decide whether a denial should be corrected, appealed, escalated to the payer, or reviewed for write-off?
- Walk me through an underpayment or paid-versus-expected variance you investigated.
- Which worklists, reports, or queue views do you use to spot patterns across claims?
- How do you explain a root-cause finding to operational staff who do not work denial codes every day?
Then score the substance of the answer, not the confidence of the delivery.
| Interview signal | Strong answer | Weak answer |
|---|---|---|
| Problem solving | Names the cause, evidence, corrective action, owner, and result | Describes fixing one claim with no broader analysis |
| Operational awareness | Connects denials to intake, coding, edits, or payer configuration | Treats each issue as isolated |
| Communication | Explains clearly, uses specific examples, and tailors the message to the audience | Relies on vague billing terms and generalities |
| Prioritization | Focuses on high-value denial categories and repeat defects | Works every account the same way regardless of yield |
Reference checks should test the same thing. Ask former managers whether the candidate reduced repeat errors, improved appeal outcomes, or helped another team correct a workflow problem. A person who closes tickets quickly may still miss the larger revenue issue.
Hiring improves when leaders stop rewarding time in seat by itself. Analytical maturity, financial judgment, and the ability to convert claim findings into operational fixes are what make this role pay for itself.
The Executive Decision Hiring In-House vs Outsourcing to a Partner
Executives often frame this as a staffing choice. It is a revenue protection choice. The question is who will identify repeat defects, assign ownership, and stop the same claim failures from hitting cash month after month.
By the time this reaches the leadership table, the organization usually has a pattern problem, not a single-person gap. Denials keep returning. A/R ages for reasons no one has fully isolated. Teams work accounts, but the same issues keep reappearing because no one has enough time or analytical depth to trace them back to registration, coding, payer setup, or follow-up workflows.
Current job descriptions reflect that shift. The role now centers on root-cause analysis, workflow redesign, system testing, error identification, remediation tracking, and dispute trend reporting. In practice, that makes the medical claims analyst closer to an operations analyst than a processor, especially in larger or multi-state organizations, as seen in this claims research analyst role focused on remediation and system issues.
Where in-house works best
An internal analyst makes sense when payer behavior is fairly stable, claim volume is predictable, and leaders want tight day-to-day coordination with clinical, coding, and front-desk teams. In that setup, the analyst can spot defects quickly and walk directly to the people who can fix them.
In-house is usually the better fit when:
- Your workflows are highly practice-specific and depend on local judgment that is hard to document fully
- Physicians or practice leaders want direct access to the person investigating reimbursement variances
- Your reporting structure is already disciplined and the analyst will have usable data, clear escalation paths, and accountable department owners
The trade-off is concentration risk. If one analyst holds the logic behind payer edits, appeal strategy, and denial categorization, turnover or leave can slow cash recovery fast. I have seen practices hire a strong analyst, then lose momentum because too much knowledge stayed in one person's inbox and worklists.
Where an external partner has the edge
Outsourcing tends to work better when the problem is broader than one hire can solve. That includes multi-site variation, uneven staff performance, fluctuating volume, or denial categories that cut across registration, coding, billing, and payer follow-up.
An external partner has the advantage when:
- Claim volume swings and staffing up and down internally would be slow or costly
- Denials span multiple departments and leadership needs a group that can coordinate findings across teams
- Specialized support is missing in payment posting, A/R follow-up, benefit verification, or denial management
- Executives need consistent reporting on patterns, defect sources, and unresolved leakage without building the full structure internally
Clarity is one example of this model. The company provides healthcare revenue cycle management support that includes claim submission, payment posting, A/R follow-up, denial management, and KPI review. That matters when a practice needs claims analysis built into the broader operating workflow, not isolated in a single job title.
Outsourcing only works when the partner does more than clear queues. The partner has to connect claim defects to operational causes, quantify the financial effect, and push corrective action back into the workflow.
A practical decision lens for leadership
Cost matters, but coverage quality matters more. A cheaper option loses value quickly if repeat denials stay unresolved, underpayments are not escalated, or staff keep reworking preventable defects.
Use this comparison to frame the decision:
| Decision factor | In-house analyst | Outsourced partner |
|---|---|---|
| Day-to-day control | High | Shared governance |
| Scalability | Limited by headcount | Easier to expand or reduce |
| Breadth of expertise | Depends on the individual hire | Broader team experience across payers and workflows |
| Continuity | Exposed to turnover and leave | More stable if the partner is staffed correctly |
| Speed to impact | Slower if training and reporting need to be built | Faster if process discipline already exists |
| Cross-functional reach | Strong if internal leaders cooperate | Stronger when neutral outside review is needed |
For stable organizations with clean processes and strong management discipline, an internal analyst can produce excellent returns. For organizations with recurring denials, weak ownership across departments, or inconsistent reporting, a partner model often fixes leakage faster because it brings capacity, structure, and pattern recognition at the same time.
The wrong move is treating this as a simple labor decision. The right move is choosing the model that will reduce rework, shorten time to payment, and prevent known defects from repeating.
Secure Your Revenue Cycle with an Expert Partner
A medical claims analyst should never be viewed as overhead. The role protects reimbursement integrity, exposes broken workflows, and gives leadership a clearer picture of where cash is leaking out of the system.
That matters because most revenue-cycle damage doesn't come from dramatic failure. It comes from repeated small misses. An authorization error that keeps recurring. A payer edit mismatch that nobody escalates. A denial category that gets worked repeatedly but never solved at the source. Those problems don't always look urgent on day one. Over time, they absorb staff capacity and distort financial performance.
Executives need more than claim handling. They need a process that can identify patterns, assign accountability, and turn findings into operational change. Sometimes that means hiring a sharp internal analyst. Sometimes it means using outside support to cover capability gaps, stabilize workflows, or manage larger portions of the revenue cycle.
The right path depends on your volume, complexity, staffing model, and tolerance for operational risk. What shouldn't be optional is analytical coverage. If no one owns denial root cause, paid-versus-denied analysis, discrepancy investigation, and follow-up discipline, your organization is relying on luck.
The practical move is to assess your current setup thoroughly. Look at where denials repeat, where handoffs break, where payment discrepancies stay unresolved, and where staff spend time on rework instead of prevention. That review usually makes the next step obvious.
If you want a clear view of where your revenue cycle is leaking and what to do about it, schedule a complimentary consultation with Clarity. The team can review your current workflows, identify gaps in claims analysis and denial management, and propose a customized approach that fits whether you need full revenue cycle support or targeted help in specific billing functions.
One response
[…] performance matters too. Readers who want a window into that side of healthcare operations may find Clarity's medical claims analyst strategy useful because it shows how administrative rigor connects to clinical business […]