A behavioral health practice with the published 2024 average denial rate of 11.8% is losing nearly 12 out of every 100 claims to payer edits, while high-performing practices report denial rates below 5%, according to behavioral health RCM benchmark data. That should change how you think about CMS behavioral health CPT denials.
This isn't just a billing nuisance. It's a cash-flow problem, an operations problem, and often a front-end discipline problem. The revenue cycle for CMS behavioral health CPT denials reveals an answer bigger than a list of denial codes. It's the full path from scheduling and insurance verification to coding, payer adjudication, posting, and follow-up. When that path breaks, revenue stalls.
Most practice owners spend too much time asking how to appeal denials. The better question is which denials should never happen in the first place, and which ones are worth working immediately before they age into low-probability receivables.
Table of Contents
- The Financial Lifeline of Your Practice Demystifying the Revenue Cycle
- Mapping the Journey The 7 Stages of the Behavioral Health Revenue Cycle
- The Denial Trap Why Behavioral Health Claims Are Rejected So Often
- From Guesswork to Insight Key Metrics for RCM Performance
- The Playbook for Prevention How to Systematically Reduce Denials
- Is It Time for a Partner Evaluating Your Need for RCM Support
- Take Control of Your Financial Health Today
The Financial Lifeline of Your Practice Demystifying the Revenue Cycle
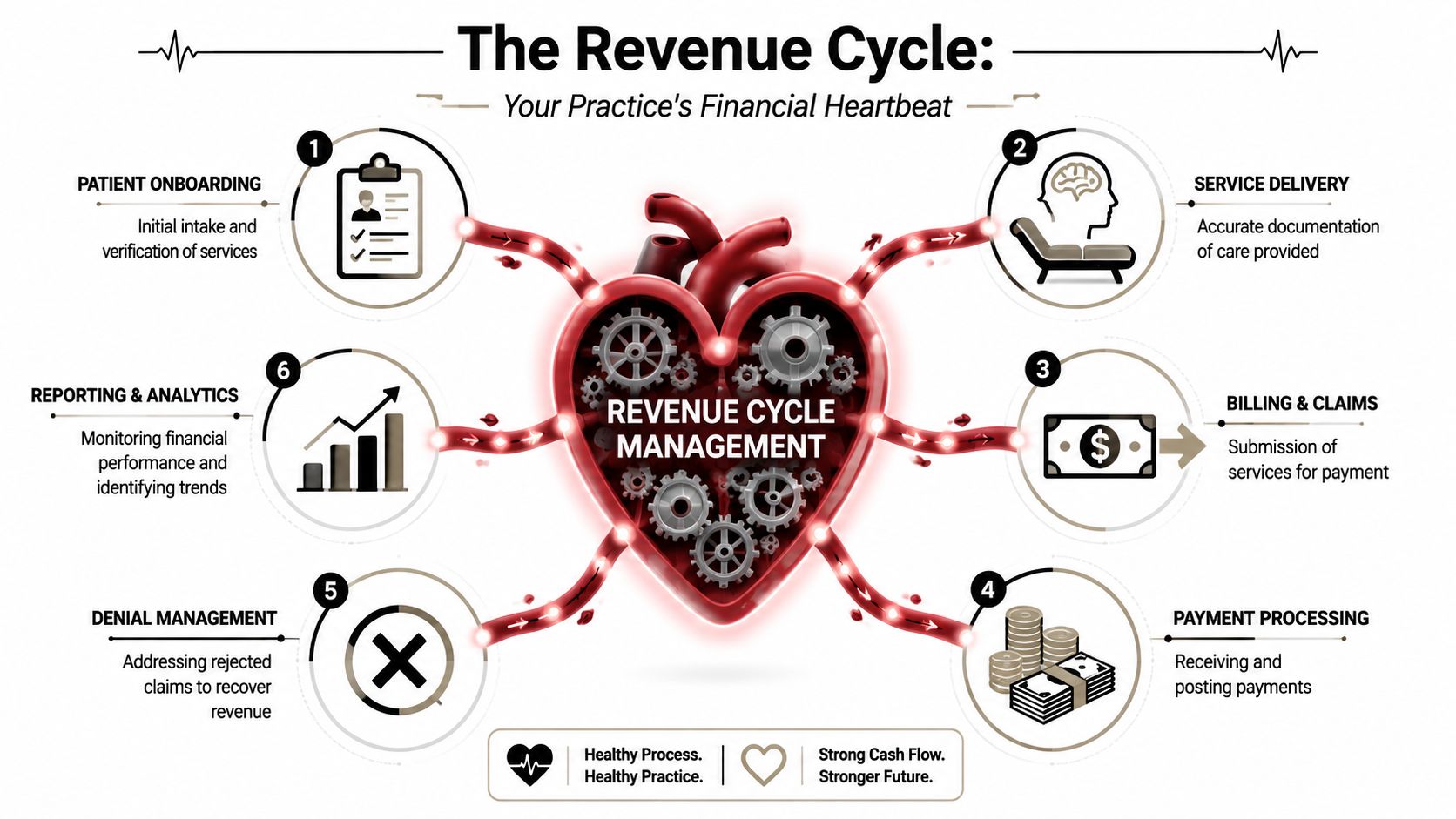
The revenue cycle is the financial heartbeat of a behavioral health practice. It's not a billing department task that starts after the session. It starts when a patient calls, fills out intake forms, or gets scheduled. It ends only when every valid dollar is collected, posted, reconciled, and resolved.
A simple way to understand it is as a relay race. One person registers the patient. Another verifies coverage. Someone confirms authorization requirements. The clinician documents the service. Coding converts the encounter into billable language. Billing sends the claim. Follow-up handles the payer's response. If anyone drops the baton, the claim may still go out, but payment often won't come back.
Why behavioral health revenue cycle work is different
Behavioral health creates tighter links between operations and reimbursement than many owners expect. A missed mental health carve-out, an expired authorization, or a note that doesn't support the billed session length can undo an otherwise legitimate encounter.
That is why the phrase what is the revenue cycle CMS behavioral health CPT denials really points to one issue. Denials are usually not isolated payment events. They are evidence that the upstream process wasn't controlled tightly enough.
Practical rule: If your team finds a denial after claim submission, assume the real fix probably sits earlier in the workflow.
Billing is only one segment of the process
Owners often say, "My billing team is following up." That's good, but it's incomplete. A healthy revenue cycle includes:
- Patient intake discipline: Correct demographics, plan details, and benefit intake before the first visit.
- Coverage validation: Verifying that the payer, product, and behavioral health administrator are the right route.
- Clinical support for billing: Notes that support time, service type, and medical necessity.
- Financial controls: Payment posting, reconciliation, denial tracking, and management reporting.
If you view revenue cycle work only as claim submission, you'll keep paying to repair avoidable mistakes. If you view it as an end-to-end operating system, you can stop a large share of denials before they ever reach the payer.
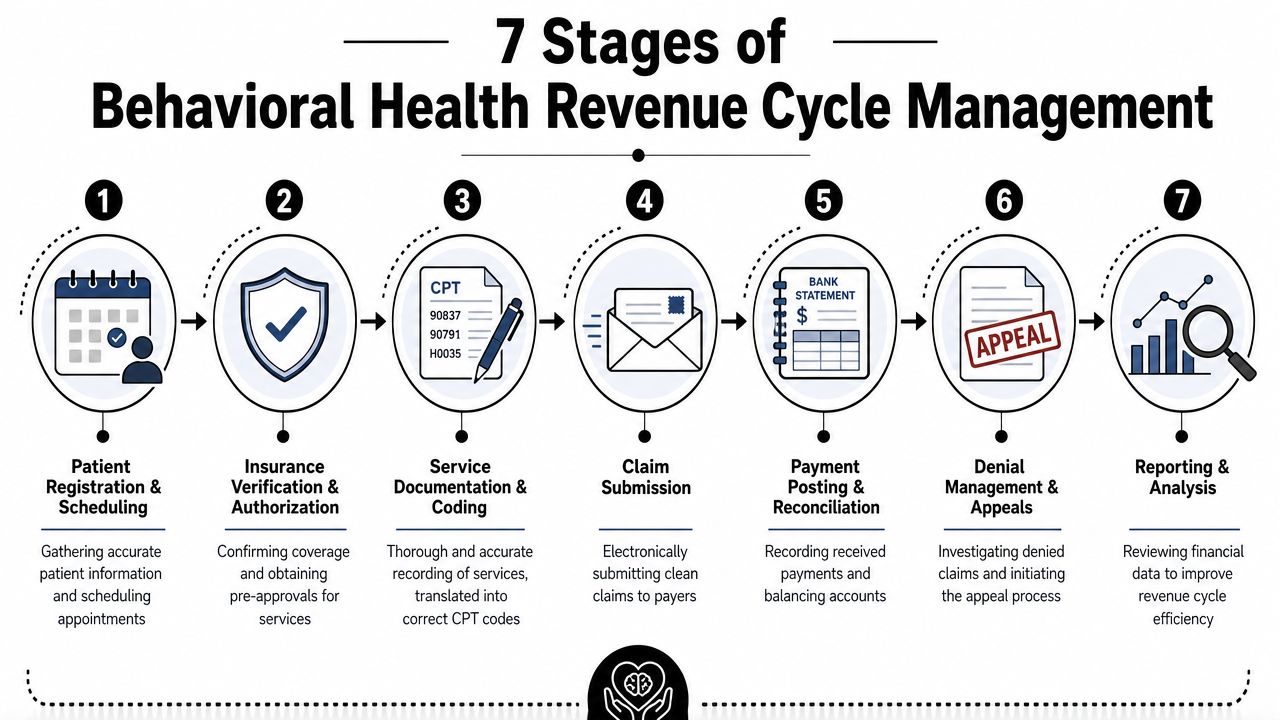
Mapping the Journey The 7 Stages of the Behavioral Health Revenue Cycle
Most revenue leaks become obvious once you map the claim's path from first contact to final resolution. In behavioral health, each handoff carries its own risk because payer requirements, documentation standards, and time-based coding rules all intersect.
A good working knowledge of claim adjudication in the payer workflow also helps here, because many practice owners don't see where payer edits, policy checks, and payment logic interrupt the process.
A relay race with seven handoffs
1. Pre-registration
This happens before the patient is seen. Staff collect demographics, insurance details, referral information, and the practical facts that affect billing later. In behavioral health, a common miss is incomplete subscriber information or assuming the medical plan also manages behavioral health benefits.
2. Eligibility and benefits verification
This step confirms active coverage and checks what the plan will pay for. Practices often verify that insurance is active but fail to verify the behavioral health side of the benefit, including carve-out routing, deductible exposure, or whether the specific service category is covered.
3. Prior authorization
Many practices often lose money without realizing it. The team must confirm whether authorization is required, for which service, for how many units or visits, and for what date range. If those details aren't logged cleanly inside the practice management system or EHR, staff may keep scheduling services after approval has expired.
4. Charge capture and CPT coding
After the visit, the service must be translated correctly into billable codes. In behavioral health, that means the documentation, the session length, and the CPT code all have to align. If a clinician documents one duration but billing selects another psychotherapy code, the claim is vulnerable.
Where practices usually lose control
5. Claim submission and scrubbing
A clean claim isn't just a claim with the right patient and provider information. It also needs the correct payer path, authorization data when required, appropriate diagnosis support, and payer-specific formatting. Clearinghouse edits help, but they don't catch every behavioral health rule.
6. Payment posting and reconciliation
Once the payer responds, the practice posts payments, adjustments, and denials. This isn't clerical cleanup. It's where patterns become visible. If one payer repeatedly denies for authorization, modifier logic, or eligibility, the posting team should surface that pattern to leadership quickly.
7. A/R follow-up and denial management
This final stage is where the practice decides whether it recovers revenue or lets it age into write-offs. Effective teams don't work every denial the same way. They classify denials, identify root causes, and push fixes upstream so the same defect doesn't keep returning.
The strongest revenue cycle teams don't celebrate heroic appeals. They build workflows that make fewer appeals necessary.
Here is the operational view owners should use:
| Stage | Core objective | Common behavioral health pitfall |
|---|---|---|
| Pre-registration | Start with accurate patient and plan data | Incomplete insurance data |
| Eligibility verification | Confirm behavioral health coverage path | Missing carve-out details |
| Prior authorization | Capture valid approval before service | Expired or mismatched auth |
| Charge capture and coding | Match note, time, and CPT selection | Session-length mismatch |
| Claim submission | Send a clean, payer-ready claim | Missing edits or wrong payer route |
| Payment posting | Record results accurately | Denial reasons not categorized |
| A/R and denial follow-up | Recover cash and prevent recurrence | Working old denials too late |
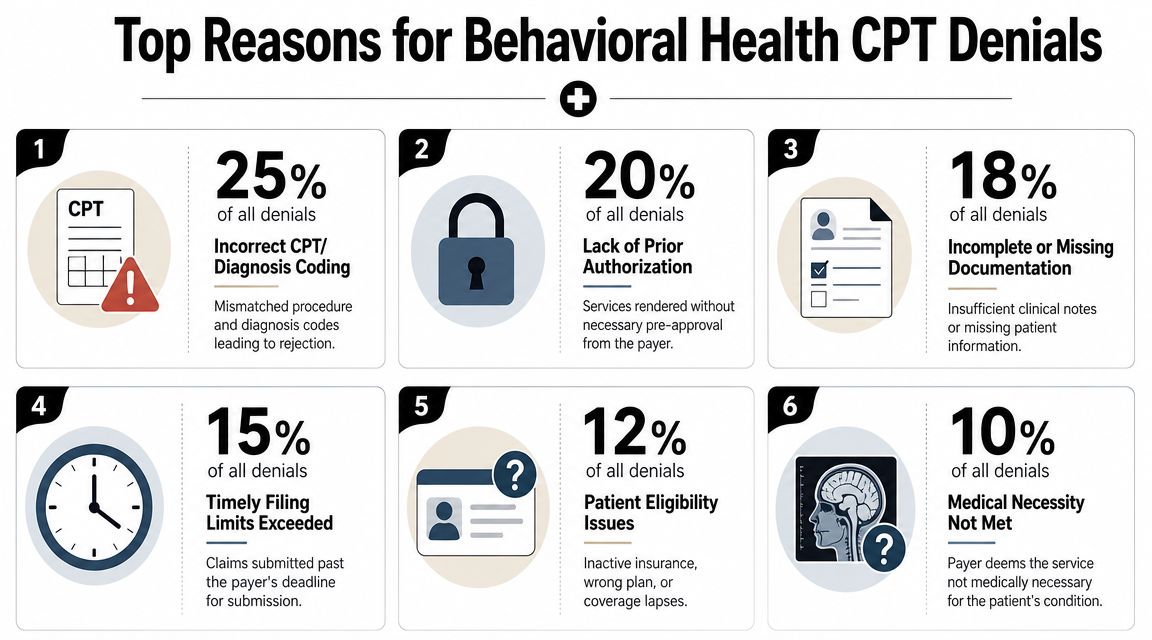
The Denial Trap Why Behavioral Health Claims Are Rejected So Often
Behavioral health claims are not denied more often by accident. The specialty is structurally more exposed to denials because billing depends on precise time-based services, stronger documentation support, and more payer-specific authorization rules.
One analysis reported that behavioral health and addiction treatment centers can face denial rates 85% higher than other medical specialties, and mental health denial rates have been reported between 15% and 25%, compared with 8% to 12% in general medicine. The same analysis estimated each denied claim costs $25 to $62 to rework and cited an average reimbursement of $115 per outpatient therapy claim, as outlined in this behavioral health billing denial analysis. That economics problem is why denials cannot be treated as routine back-office friction.
Why behavioral health gets hit harder
The first issue is authorization complexity. Behavioral health benefits are often carved out, managed separately, or subject to strict pre-service review. A front-desk team may think the patient is "verified" while the actual behavioral health administrator was never contacted.
The second issue is time-based CPT exposure. If a claim uses a psychotherapy code that doesn't match the documented session length, the payer has a simple path to deny or downcode it. Behavioral health uses these timing distinctions constantly, which makes process discipline absolutely essential.
Here is a practical walkthrough on the topic for teams that want a deeper operational view of behavioral health CPT billing denials.
The denial patterns that matter most
After the opening diagnosis, bring your team back to the repeat offenders:
- Authorization failures: Missing prior auth, expired visits, or approval for one service with billing submitted for another.
- Eligibility and routing errors: Coverage may be active, but the claim still goes to the wrong payer or wrong behavioral health entity.
- Documentation gaps: The note may be clinically acceptable yet still fail to support medical necessity or the billed code.
- CPT mismatch: Session duration, service type, modifier use, and payer policy don't line up.
Later in your workflow review, use training content like this to align staff and providers:
A denied therapy claim isn't just lost time. In many cases, the rework cost alone eats a meaningful share of the original reimbursement.
What doesn't work is attacking these denials one by one with generic appeal letters. What works is identifying which failure point is repeating, then fixing the upstream handoff that created it.
From Guesswork to Insight Key Metrics for RCM Performance
A small shift in collections can put a behavioral health practice under real strain. If even a modest share of claims is denied, delayed, or underpaid, the impact shows up fast in owner draws, payroll timing, and therapist compensation.
That is why leadership needs a short scorecard. Not a giant dashboard. A few numbers, reviewed consistently, will show where cash is leaking and which problems deserve attention first.
The four metrics that deserve leadership attention
Claim denial rate
This is the percentage of claims payers reject after submission. Track it by payer, location, provider type, and CPT family. A single blended rate hides the underlying issue.
Claim Denial Rate = Denied claims / Total submitted claims
If this number rises, do not start with appeals volume. Start by asking which denial categories are creating the largest dollars at risk. In many behavioral health groups, a handful of front-end misses produce most of the rework. Prior authorization lapses, eligibility mistakes, carve-out routing errors, and coding mismatches usually cost more than isolated payer disputes.
Clean claim rate
This measures how often claims are accepted on the first pass, without edits or rejections.
Clean Claim Rate = First-pass accepted claims / Total submitted claims
This metric is one of the fastest ways to judge front-end discipline. A weak clean claim rate usually points to intake, registration, auth tracking, or coding setup problems. If the rate drops, billing staff often get blamed first. In practice, the root cause often sits earlier in the workflow.
Days in A/R
This shows how long it takes to turn completed services into cash.
Days in A/R = Total A/R / Average daily charges
When days in A/R climb, the issue is rarely just payer speed. It often means denied claims are aging, follow-up is inconsistent, or small posting problems are stalling larger balances. Owners should also separate current A/R from 90-plus-day A/R. Old money and collectible money are not the same thing.
A simple scorecard for owners and CFOs
Net collection rate shows how much of the revenue you were entitled to collect made it into the bank.
Net Collection Rate = Payments / Allowed amount
Used correctly, this metric keeps teams from celebrating charges instead of cash. For a closer breakdown, this guide on net collection rate in healthcare RCM explains how practice leaders use it to spot write-off problems, underpayments, and weak follow-up.
Use these four metrics together:
| Metric | Formula | What it tells you |
|---|---|---|
| Claim denial rate | Denied claims / Total claims | How much preventable friction is hitting your claims |
| Clean claim rate | First-pass accepted claims / Total claims | Whether claims are leaving your system correctly |
| Days in A/R | Total A/R / Average daily charges | How fast services turn into cash |
| Net collection rate | Payments / Allowed amount | How much collectible revenue you actually keep |
A pattern matters more than any single number.
If denial rate is rising while clean claim rate is falling, the practice has a front-end process problem. If denial rate is stable but days in A/R and net collection rate worsen, the practice likely has a follow-up, posting, or underpayment problem. That distinction matters because it changes where you put management time.
I tell owners to review these metrics in dollar terms, not just percentages. Twenty denials for small balances may be annoying. Five denials tied to high-dollar psych testing, IOP, or recurring therapy authorizations may be the issue that deserves action this week. That is how denial management becomes financially useful instead of just operationally busy.
The Playbook for Prevention How to Systematically Reduce Denials
The highest-return denial strategy in behavioral health is prevention. Not appeals. Not work queues. Not heroic end-of-month cleanup.
Authorization control is the biggest lever. In behavioral health revenue cycle management, missing or expired prior authorizations, carve-out routing errors, incorrect time-based CPT selection, eligibility lapses, and timely-filing problems are reported as the main causes of roughly 80% of behavioral health denials, according to this behavioral health authorization and denial prevention review. That should reshape where you put staff attention.
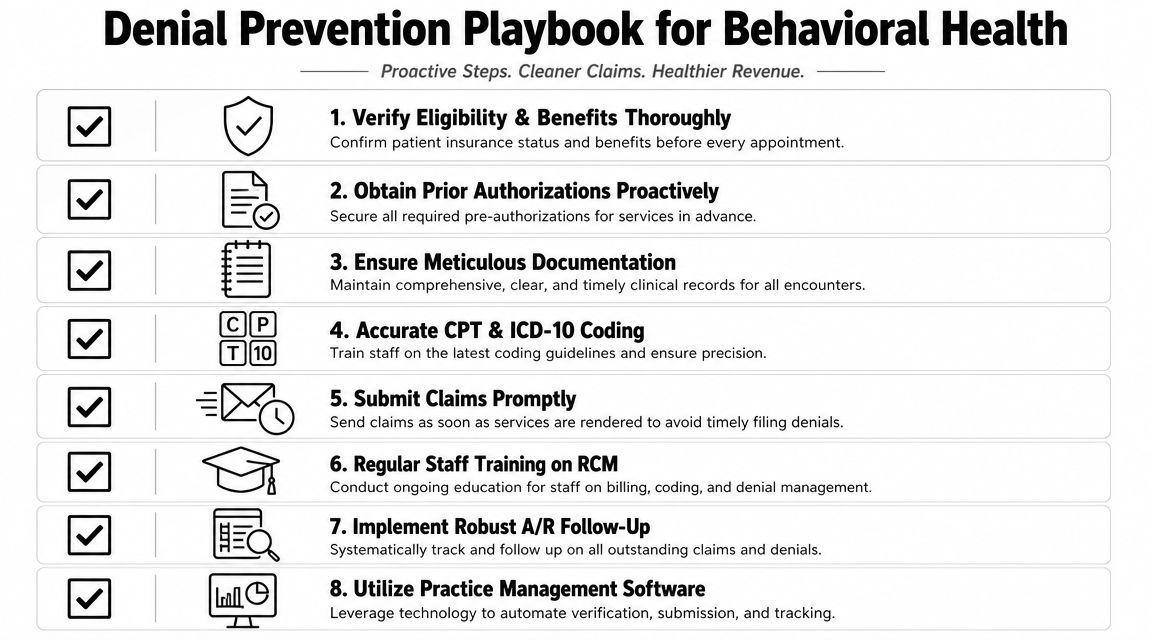
Fix the front end first
A practical prevention playbook looks like this:
- Verify the actual behavioral health payer path: Don't stop at "coverage active." Confirm whether behavioral health is carved out and where claims must go.
- Track authorization like inventory: Record auth number, service type, approved units or visits, and expiration date in one place your schedulers and billers can both see.
- Force note-to-code alignment: Build EHR templates that require clinicians to document the facts billing needs, especially session duration and service type.
- Use clearinghouse edits intelligently: Scrub for missing data, but also review recurring payer-specific edits that your standard setup may not catch.
- Submit quickly: Fast submission shortens the feedback loop. You learn about payer defects while the encounter is still fresh and easier to correct.
What works and what usually fails
What works is standardization.
Create short internal job aids for front desk, utilization review, clinicians, and billing staff. A one-page psychotherapy coding reference, a daily auth expiration report, and a payer-routing checklist usually outperform long policy manuals that nobody uses.
What fails is fragmented ownership. If one team verifies coverage, another tracks authorizations on a spreadsheet, clinicians document however they prefer, and billing discovers the mismatch two weeks later, denials are predictable.
Use these dos and don'ts as operating rules:
Do
- Audit scheduling against authorization status: Prevent unapproved visits before they occur.
- Train clinicians on billing consequences: They don't need to become coders, but they do need to understand how documentation supports payment.
- Work rejection reports daily: Catch front-end data issues before they convert into aged denials.
- Sort denials by root cause: Group by auth, eligibility, documentation, coding, filing, and payer-routing defects.
Don't
- Don't rely on memory for auth dates: Manual recall always breaks at scale.
- Don't appeal everything equally: Some denials are better fixed at process level than worked repeatedly claim by claim.
- Don't assume Medicare logic stays isolated to Medicare: Many payer policies mirror CMS-style coding expectations.
- Don't separate finance from operations: Denials start in workflow, not in the accounting ledger.
The fastest way to improve collections is often to stop creating bad claims, not to get better at arguing over them later.
Is It Time for a Partner Evaluating Your Need for RCM Support
Some practices can tighten their revenue cycle in-house. Others have already crossed the line where internal bandwidth, training gaps, or lack of reporting discipline make outside support the better financial choice.
A practical self-assessment
You likely need help if several of these are true:
- Your team can't explain the top denial reasons clearly: If leadership hears only "insurance is denying a lot," the reporting layer is too weak.
- Authorizations are tracked in disconnected places: Spreadsheets, email threads, sticky notes, and EHR comments are a setup for missed visits and lost claims.
- Clinicians and billers blame each other: That usually means there is no clean operating standard connecting documentation to charge capture.
- Old denials sit untouched: Once denials age, recoverability drops and staff effort becomes less productive.
- Cash flow feels unpredictable: When deposits swing but leadership can't tie the variance to payers, services, or denial categories, the practice is managing by reaction.
Behavioral health guidance notes that denials more than 60 days old have significantly lower recovery rates, and denial rates in behavioral health can run 25% to 30%. The same guidance highlights the operational need to prioritize denials by payer, denial code, and service line, as explained in this behavioral health denial aging and prioritization discussion.
Where outside RCM support changes the outcome
An experienced RCM partner usually changes the result in three areas.
First, they impose process discipline. Eligibility checks, auth controls, coding review, claim edits, and follow-up workflows become standardized instead of personality-driven.
Second, they improve denial prioritization. Not every denial deserves the same labor. A smart team works the denials with the best cash impact and recovery potential first, instead of letting staff burn time evenly across the queue.
Third, they create management visibility. Owners and CFOs stop hearing anecdotes and start seeing patterns by payer, service type, and workflow defect.
If your internal team is talented but overloaded, support doesn't have to mean handing over everything. Some practices need full-service management. Others need focused help with eligibility verification, payment posting, or A/R and denial follow-up. The right model is the one that removes the bottleneck without adding operational chaos.
Take Control of Your Financial Health Today
Behavioral health revenue cycle work is complicated because payment depends on operational precision. It isn't enough to provide good care. The practice has to capture the right payer, the right authorization, the right documentation, and the right CPT logic in the right order.
CMS coding rules are a good final reminder. For psychiatry and psychotherapy billing, 90832, 90834, and 90837 are core psychotherapy codes, while 90885, 90887, and 90889 are incidental and not separately payable. A mismatch between documented session length, service type, and submitted CPT code can trigger denials or nonpayment under Medicare and payer policies that mirror CMS logic, as outlined in the CMS psychotherapy coding article.
If you want a practical answer to what is the revenue cycle CMS behavioral health CPT denials, it's this. Your revenue cycle is the full financial journey of each patient account, and CPT denials are the visible symptom when that journey breaks. Fixing the issue starts with prioritizing front-end prevention, measuring the right KPIs, and working denials based on financial impact instead of habit.
You don't need more billing noise. You need cleaner intake, tighter authorization control, stronger documentation discipline, and better denial triage.
If your behavioral health practice needs a clearer picture of where revenue is leaking, schedule a complimentary consultation with Clarity. Clarity can review your current revenue cycle, identify breakdowns in verification, authorization, coding, payment posting, and denial follow-up, and recommend a support model that fits your team. Whether you need full-service RCM or help in a few critical gaps, the goal is the same. Protect cash flow, reduce avoidable denials, and give your clinicians more room to focus on patient care.
No responses yet