Healthcare organizations in the United States spend an estimated $19.7 billion annually fighting for reimbursements they already earned, and some sources place hospital spending on claim denial appeals at approximately $20 billion per year (Qualify Health on medical revenue recovery). That figure changes the way medical revenue recovery should be viewed. This isn't a billing-office nuisance. It's a balance-sheet issue.
Most finance leaders already know cash is slipping somewhere. What they often need is a better model for where it leaks and how to close the loop. Effective medical revenue recovery starts before the claim is sent, continues through denial follow-up, and doesn't end when an account hits zero balance. If the claim was underpaid, misclassified, or shorted against contract terms, the revenue cycle still has work to do.
Table of Contents
- Why Lost Revenue Is a Solvable Problem
- Decoding Medical Revenue Recovery
- Pinpointing Common Sources of Revenue Leakage
- A Four-Step Framework for Effective Recovery
- Measuring Success with Key Recovery KPIs
- Real-World Recovery Workflows and Outcomes
- When to Partner with a Revenue Cycle Management Firm
Why Lost Revenue Is a Solvable Problem
Revenue loss in healthcare rarely comes from one catastrophic error. It usually comes from repeatable process defects. An eligibility miss at registration. A prior auth not attached. A coding mismatch that triggers denial. A claim that was denied correctly but never worked again. A payment that posted cleanly but was still short.
That matters because repeatable defects are manageable defects. When leaders treat medical revenue recovery as a continuous operating discipline, they stop framing lost revenue as bad luck or payer behavior alone. They start tracing it to workflows, ownership gaps, and weak controls.
CFOs and practice leaders are under pressure from both sides. Reimbursement is difficult, labor is expensive, and operational complexity keeps expanding. In that environment, recovered revenue has a different value than new volume. It often comes from services already rendered, documentation already completed, and contracts already in force. The issue isn't generating demand. It's collecting what the organization has earned.
Practical rule: If a loss pattern can be categorized, it can usually be reduced.
The organizations that improve recovery don't begin by chasing every old account equally. They identify where leakage starts and who owns that step. In many cases, the fastest improvement comes from basic discipline:
- Tight registration controls so eligibility errors don't move downstream
- Clear payer-rule ownership so authorization and documentation requirements are visible before service
- Structured denial queues so denied claims aren't left to age without action
- Post-payment review logic so closed claims can still be checked for underpayment
A good recovery program also changes internal conversations. Instead of asking, "Why are denials high?" the better question is, "Which denial categories are preventable, which are appealable, and which are signs of a front-end process failure?" That distinction is where solvability starts.
Lost revenue feels inevitable when teams only see symptoms. It becomes solvable when leadership treats the revenue cycle like a control system, not a set of disconnected billing tasks.
Decoding Medical Revenue Recovery
Medical revenue recovery is best understood as a financial leak-prevention and recapture system. Collections is only one part of it. The broader job is to find where earned revenue is escaping, fix the cause, and recover what can still be collected.
Recovery is bigger than collections
A useful analogy is a leaky pipeline. If the only response is to place a bucket at the end, the organization may collect some of what spills out, but the system is still failing upstream. That's what happens when a practice relies on aged A/R work alone. Staff chase balances after the damage is done, while the same defects keep producing new leakage.
A modern recovery function covers at least three operational zones:
- Denial management, which includes triage, documentation review, appeal routing, and payer follow-up
- A/R follow-up, which keeps unpaid or partially paid claims moving instead of sitting in status limbo
- Underpayment detection, which tests whether posted payments matched contract and coding expectations
The handoff between claim submission and payer decision also matters. Teams that understand claim adjudication in healthcare usually recover faster because they know where a claim can stall, reject, pend, or short-pay before anyone labels it "just a denial problem."
Think in loops, not handoffs
What works is a loop. Registration errors inform front-desk scripts. Denial trends inform coder education. Underpayment findings inform contract review. Appeal outcomes inform documentation templates. Revenue recovery gets stronger when each downstream finding becomes an upstream correction.
What doesn't work is organizational siloing. If the billing office sees denials, coding sees edits, and operations sees patient throughput, but no one connects those signals, leakage becomes permanent. The claim may get fixed, but the process doesn't.
Closed claims can still hide missed revenue. Open claims aren't the only recovery opportunity.
That is why medical revenue recovery belongs in finance discussions, not only billing meetings. It affects cash timing, margin protection, labor utilization, and forecasting accuracy. A healthy revenue cycle isn't just one that submits claims. It's one that learns from every claim outcome and adjusts the process before the next dollar leaks out.
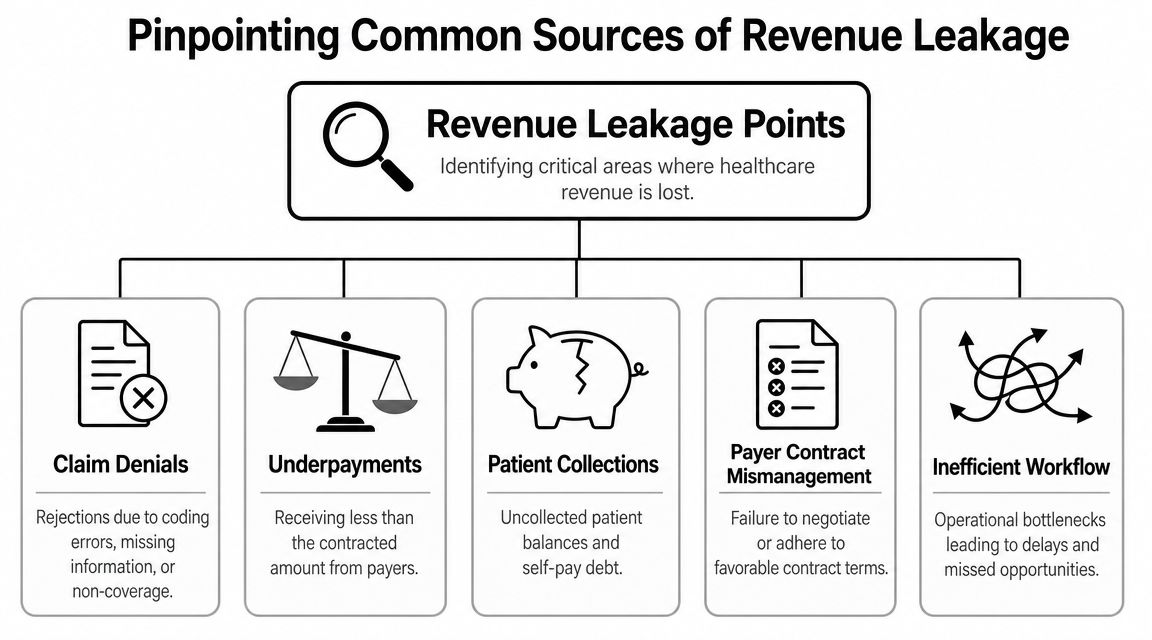
Pinpointing Common Sources of Revenue Leakage
Most organizations don't have one leak. They have a pattern of small leaks spread across the revenue cycle. The practical task is to locate them by stage and assign ownership.
One of the clearest warning signs of internal process failure is follow-up abandonment. According to MGMA data, about 65% of claim denials were never corrected and resubmitted (Promantra on healthcare revenue recovery). That doesn't point first to payer hostility. It points to weak routing, poor prioritization, or unclear accountability after denial.
Front-end leakage
The front end creates many of the losses that later appear as denials or patient bad debt.
Common examples include:
- Insurance verification gaps that leave inactive, secondary, or incorrect coverage undiscovered
- Missing authorizations for services that require payer approval before treatment
- Registration errors in demographics, subscriber details, or plan sequencing
- Poor patient financial clearance when responsibility isn't communicated early
These errors are expensive because they contaminate every downstream step. A clean appeal can't fully rescue a claim that should never have left the front desk in that condition.
Mid-cycle leakage
Mid-cycle leakage often sits between clinical work and bill creation. Finance leaders don't always see it directly because it looks like "coding delay" or "billing rework," but the root problem is usually documentation and charge integrity.
Watch for these patterns:
- Coding mismatches between documentation and billed services
- Missed charges from incomplete charge capture workflows
- Late edits that push claims past timely filing windows
- Inconsistent modifier use that causes avoidable payer rejections
A denial trend is rarely just a denial trend. It usually reflects registration, documentation, coding, or workqueue design upstream.
Back-end leakage
The back end is where organizations often discover the problem, but not where it began. That's why back-end teams need both recovery discipline and escalation authority.
The biggest trouble spots are usually operational, not mysterious:
| Leakage point | What it looks like in practice | Why it persists |
|---|---|---|
| Unworked denials | Claims sit in queues without correction or appeal | No owner, poor prioritization |
| Aging A/R | Claims pend or rebill repeatedly without resolution | Follow-up isn't scheduled tightly |
| Underpayments | Payment posts and account closes, but reimbursement is short | Zero-balance claims aren't reviewed |
| Patient balances | Statements go out, but collectability declines quickly | Financial responsibility wasn't set early |
If you're diagnosing your own operation, start with denial categories, aging buckets, payer-specific rejection reasons, and zero-balance exceptions. Those views usually expose whether the problem is front-end accuracy, coding quality, follow-up execution, or contract payment integrity.
A Four-Step Framework for Effective Recovery
High-performing recovery programs do more than overturn denials. They create a closed-loop process that prevents repeat errors, recovers missed dollars, and verifies that posted payments match contract terms.
A workable framework has four parts: identify, analyze, act, and optimize. Used consistently, it turns revenue recovery from a reactive billing task into an ongoing financial control.
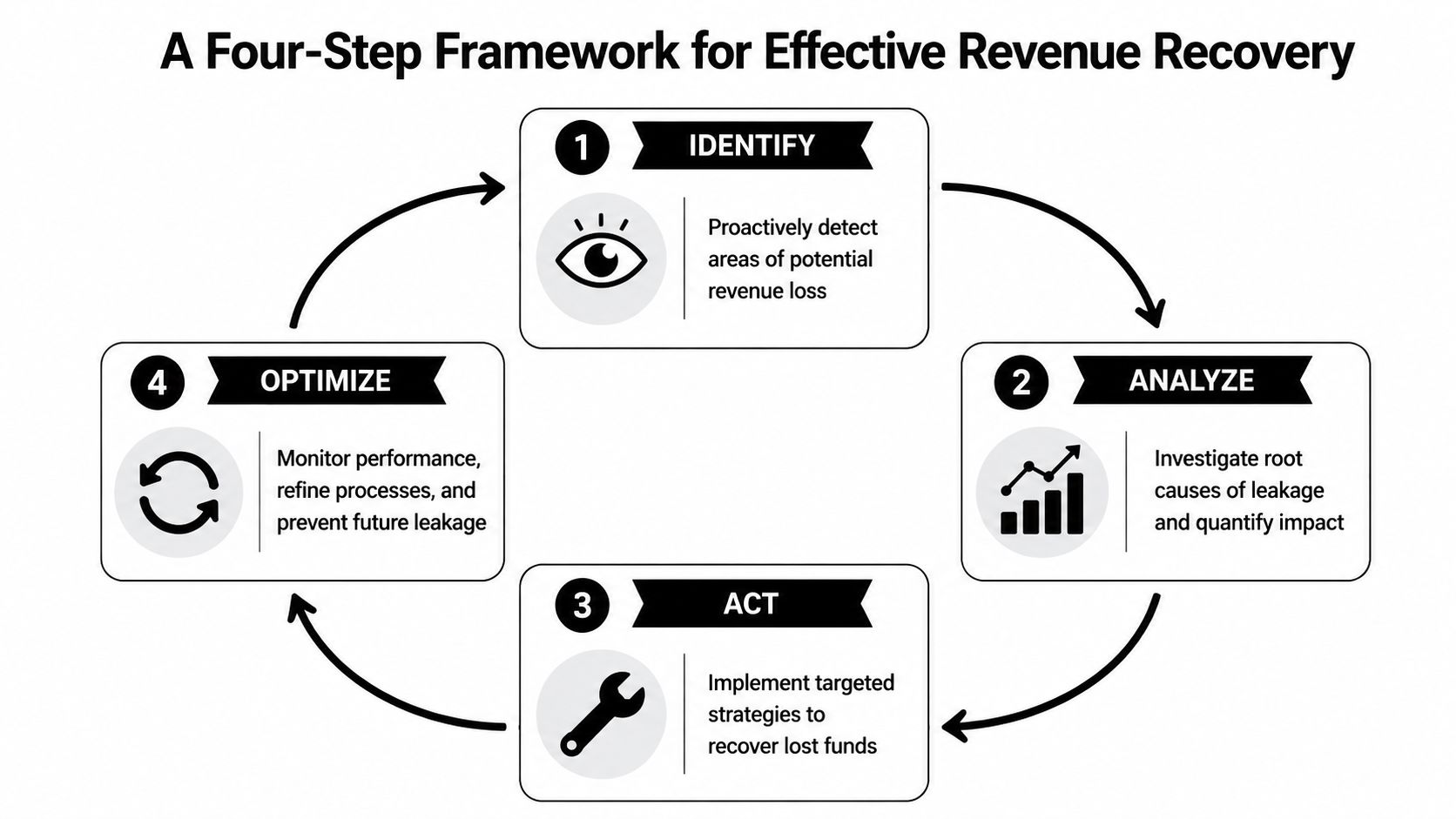
Step 1 identify what routine reporting misses
Start with focused audits tied to dollars at risk. Review denial clusters by payer and service line, edits that recur after rebilling, aging patterns that suggest stalled follow-up, and closed claims with payment variances that do not fit the expected contract outcome.
Post-payment review belongs in this step. A zero balance only confirms the account was closed in the system. It does not confirm full reimbursement. Reviewing zero-balance claims often exposes underpayments, code-level reimbursement errors, and contract logic issues that standard denial reports never catch, which is why EnableComp's revenue recovery overview calls out underpayment detection as part of the recovery process.
Priority findings usually include:
- Repeat denials concentrated in one payer rule or service line
- Appeals that fail at the same documentation requirement
- Closed claims with likely short payment
- Accounts with high touch counts and no resolution
A team that can see those patterns early can decide whether the problem is isolated, systemic, or contract-driven.
Later in the workflow, teams need to standardize action. This walkthrough is useful context for leaders aligning staff around recovery operations:
Step 2 analyze by root cause and recoverability
Every claim should not receive the same level of effort. Segment work by root cause, payer behavior, documentation burden, expected reimbursement, and probability of recovery.
Operating discipline protects margin. A low-dollar denial with weak documentation support may cost more to appeal than it can return. A high-dollar underpayment across a repeated payer pattern deserves immediate attention because the same variance may be affecting hundreds of closed claims. Strong teams score accounts by financial impact first, then assign the right path: correction, appeal, rebill, escalation, or process change.
Teams that make this shift stop treating recovery as queue cleanup. They start treating it as yield management.
Step 3 act with disciplined follow-up
Recovery succeeds or fails in execution. Workqueues need clear ownership, aging rules, due dates, and escalation paths by payer. If an account moves between billing, coding, and operations without a deadline, recovery slows and filing risk increases.
Four practices improve results fast:
- Assign one accountable owner for each claim until resolution
- Use standard appeal packets for denial categories that repeat
- Set follow-up intervals based on payer response times and status codes
- Log each touch clearly so the next staff member continues the work instead of restarting it
For leadership, the financial lens matters as much as the operational one. Tracking recovery activity against net collection rate performance in healthcare RCM helps show whether follow-up is improving collectible revenue.
Step 4 optimize the upstream process
Recovery should change future claim performance. If appeals repeatedly require one missing physician statement, update the documentation checklist. If eligibility errors keep surfacing, tighten registration scripts and verification rules before the claim is created. If underpayments cluster under one contract term, adjust payment posting edits and audit those zero-balance accounts on a set schedule.
That is the full lifecycle of recovery. Prevent avoidable leakage before claim submission. Recover open denials and aged accounts with discipline. Then audit paid claims for underpayments and feed the findings back into front-end, coding, billing, and contract workflows.
Organizations also need to decide which functions belong in-house and which need outside support. Some groups keep day-to-day billing internally and bring in specialized help, such as Clarity's specialized healthcare revenue cycle support, for benefit verification, payment posting, or focused billing operations support.
Measuring Success with Key Recovery KPIs
Finance teams need a small set of metrics that reveal whether recovery work is improving cash performance or just creating activity. The most useful KPIs aren't exotic. They're operational indicators that connect prevention, recovery, and net reimbursement quality.
According to an industry guide, healthy revenue cycle benchmarks include Days in Accounts Receivable of 30 to 40 days, a Clean Claim Rate of 90% or higher, a final denial rate below 5%, and a Net Collection Ratio of 95% or higher (PRGMD on revenue recovery benchmarks).
The KPI table finance teams should actually use
| KPI | Industry Benchmark | What It Measures |
|---|---|---|
| Days in Accounts Receivable | 30–40 days | How long it takes to convert billed revenue into cash |
| Clean Claim Rate | 90% or higher | How often claims go out correctly the first time |
| Final Denial Rate | Less than 5% | How much claim volume ultimately fails after rework and appeal |
| Net Collection Ratio | 95% or higher | How much of collectible reimbursement the organization actually captures |
For leaders who want a tighter explanation of the reimbursement side, this guide to net collection rate in healthcare RCM helps frame why net collections are often a better management signal than gross billing totals.
How the metrics interact
These metrics should be read together, not in isolation. A weak clean claim rate usually drives more rework, which stretches A/R days. Higher final denials pull down net collections. Long A/R can also hide process weakness because unresolved claims stay on the books while cash lags behind.
A few practical interpretations matter:
- High A/R with decent net collections often means the team eventually gets paid, but too slowly
- Good clean claim rate with poor net collections can signal underpayment, bad follow-up, or patient balance weakness
- Low denial rate with high A/R may point to pended claims, status neglect, or payment posting delays
The best KPI set doesn't just measure output. It tells you where the process broke.
A CFO should expect every revenue-cycle meeting to tie one KPI movement to an operational cause. If the team can't explain why a metric moved, it usually means the reporting is descriptive but not actionable.
Real-World Recovery Workflows and Outcomes
The most useful way to understand medical revenue recovery is to watch a single denial pattern move through the operating model.
A common denial pattern
A behavioral health group starts seeing recurring denials tied to medical necessity documentation. The denial codes vary by payer wording, but the underlying issue is the same. The clinical note doesn't consistently include the elements the payer wants to justify the service.

The first mistake many teams make is treating each denied claim as a one-off. They correct one account, submit one appeal, and move on. The denials continue because the workflow never changed. This is especially common in specialties where documentation requirements and payer edits shift often, including patterns similar to those described in behavioral health CPT billing denials.
How the workflow changes operations
A better response is coordinated.
The audit team pulls denied claims by payer and service line and confirms the recurring documentation gap. Billing then groups those denials into a dedicated queue rather than leaving them mixed with unrelated edits. An appeal template is built around the missing support, and coders or billers route each claim back for exactly the addendum needed. A/R staff track payer acknowledgment and decision dates so the appeal doesn't disappear after submission.
At the same time, the practice changes the front-end clinical checklist. Providers get a short documentation prompt tied to the service involved. Supervisors spot-check new encounters before billing. The revenue recovery work doesn't stop at resubmission. It feeds a process correction that reduces the next batch of denials.
That's the true outcome to aim for. Not a heroic one-time clean-up, but a workflow that recovers open dollars and lowers repeat leakage. In practice, the strongest teams judge success by fewer recurring denial classes, faster claim resolution, cleaner documentation, and less manual rework across departments.
When to Partner with a Revenue Cycle Management Firm
Delayed recovery work is expensive. Every week a preventable denial sits untouched or an underpayment goes unreviewed, cash stays off the books and staff time gets spent on rework instead of clean production.
Some organizations should keep recovery in-house. That works when leadership has enough billing depth, clean ownership across departments, and the discipline to turn recovery findings into front-end process changes. A partner makes sense when the recovery cycle has broken into isolated tasks instead of one financial control loop, from eligibility and charge capture through denial follow-up and post-payment review.
Signs the in-house model is stretched
The clearest signal is not volume alone. It is repeated leakage across multiple stages of the cycle, with no one accountable for fixing the source.
Consider outside support when several of these conditions are present:
- A/R remains high and the team cannot separate delays by payer, service line, age bucket, or claim status
- Denial follow-up depends on individual staff habits rather than standard queues, deadlines, and appeal rules
- Paid claims are rarely audited for underpayment because staff is consumed by current billing and old denials
- Payer policy changes outpace internal updates to registration, coding edits, and claim submission workflows
- Leadership receives reports without root-cause analysis or a clear action plan tied to financial impact
- Ownership is split across front desk, coding, billing, and finance with no single process leader for leakage reduction
I see this pattern often. Staff are working hard, touches are high, and the same avoidable losses keep showing up month after month. That points to a process control problem, not a simple staffing shortage.
What an external partner should do
A revenue cycle management firm should improve control across the full recovery lifecycle. That includes pre-claim prevention, denial prevention, active A/R recovery, and post-payment underpayment review.
Useful support usually looks like this:
| Need | What useful support looks like |
|---|---|
| Front-end prevention | Eligibility checks, benefit validation, authorization tracking, registration quality controls |
| Mid-cycle claim quality | Charge review, claim edit resolution, timely filing protection, denial trend monitoring |
| Back-end follow-up | Claim status work, denial routing, appeal management, payment posting review |
| Post-payment recovery | Underpayment audits, zero-balance review, contract variance identification, refund risk checks |
| Flexible staffing | Full-cycle support or targeted help where the internal team has the biggest gap |
The right arrangement is rarely all or nothing. A practice may keep coding and patient access in-house but outsource denial follow-up and underpayment audits. A larger group may only need help with aged A/R cleanup, payer variance review, or temporary staffing during turnover. The trade-off is straightforward. Internal teams usually know the clinical workflow better, while outside teams often bring tighter recovery discipline, broader payer pattern recognition, and more consistent follow-through.
Clarity can review your current revenue cycle and help determine whether full-service support or targeted operational help makes more sense for your organization.
If your organization needs a clearer view of where revenue is leaking, Clarity offers a complimentary consultation to assess your current revenue cycle and recommend a customized approach, whether you need full-cycle management or support in specific functions like benefit verification, claim follow-up, and payment posting.
Prepared with the Outrank tool
One response
[…] patient billing. For practices dealing with old balances and under-collected claims, focused medical revenue recovery support can also help address revenue that already slipped […]