Most advice about net collection rate starts with a benchmark and stops there. If your number looks high, you're told the revenue cycle is healthy. That's too simplistic.
A practice can post a strong net collection rate and still leak profit through underpriced services, weak contract management, or write-offs that should have been appealed instead of closed out. If cash feels tighter than the KPI suggests, the metric isn't useless. You're just asking too little from it.
Leaders who treat net collection rate as a scoreboard often miss the operational story underneath it. Leaders who treat it as a diagnostic tool usually find the friction points faster, fix them earlier, and stabilize cash flow with less guesswork. That distinction matters if you're trying to control revenue leakage, defend margin, and make sense of why collections feel inconsistent even when the dashboard looks fine. Teams that already track broader revenue cycle management topics usually spot this sooner, because they don't isolate one KPI from the rest of the financial picture.
Table of Contents
- Why Your Net Collection Rate Is a Critical Health Metric
- How to Calculate Your Net Collection Rate
- Calculating Net Collection Rate With a Real Example
- What Is a Good Net Collection Rate
- Diagnosing and Fixing a Low Net Collection Rate
- Partnering with Clarity to Maximize Your Collections
Why Your Net Collection Rate Is a Critical Health Metric
Net collection rate matters because it tells you whether the practice is collecting the revenue it had a realistic right to collect. That makes it more useful than broad top-line billing totals and more actionable than a generic collections report.
For owners, CFOs, and physician leaders, this metric sits close to the cash question that hurts. Are we failing to collect money we earned, or are we dealing with a payer mix and fee structure issue that needs a different response? Those are not the same problem, and they shouldn't be managed the same way.
A healthy net collection rate usually points to discipline in billing, follow-up, payment posting, and patient balance recovery. A weak one often signals preventable leakage. Claims may be leaving with errors. Eligibility may be checked too late. Denials may be sitting untouched. Patient balances may be aging because statements are unclear or the handoff at check-in is weak.
Why finance leaders should care
When cash becomes unpredictable, many practices chase the wrong explanation first. They blame seasonality, staffing turnover, or payer behavior in general terms. Sometimes that's true. Often, the root issue is narrower and more fixable.
Net collection rate helps narrow the search. It gives you a way to separate collectible revenue from fantasy revenue. That distinction supports better budgeting, better provider compensation conversations, and cleaner decisions about whether to invest in staff, technology, or outside support.
A collection problem isn't always a volume problem. Often it's a process problem hiding inside allowed revenue.
Why the metric gets misused
The mistake isn't tracking net collection rate. The mistake is treating it like a trophy number. When leadership only asks whether NCR is high, staff learns to protect the number, sometimes in ways that hurt margin. Balances get written off too quickly. Small underpayments get ignored. Contract variances never get escalated because they don't immediately crush the KPI.
That's why this metric is critical. Used correctly, it reveals whether your revenue cycle is converting earned revenue into cash. Used lazily, it can reassure you while the practice gives money away.
How to Calculate Your Net Collection Rate
The basic calculation is straightforward. The actual challenge is using the right inputs and understanding what the formula excludes.
Near the start of any billing review, I explain net collection rate as your success rate on winnable revenue, not on every dollar ever billed. That's the cleanest way to understand why this metric matters more than a raw collection percentage from total charges. If your team works in billing, coding, or medical billing operations, that distinction should shape how you read every monthly report.
What the formula is actually measuring
Use this formula:
Payments / (Charges – Contractual Adjustments)
Each piece matters:
- Payments means money received. That includes payer payments and patient payments that have posted to the accounts you're measuring.
- Charges means the total amount billed for services provided during the reporting period.
- Contractual adjustments are the expected reductions tied to payer agreements. These amounts were never realistically collectible at full charge, so they should be removed before you judge collection performance.
This is why net collection rate is more meaningful than gross collection rate. Gross collection rate asks, "How much did we collect against what we billed?" Net collection rate asks, "How much did we collect against what we were entitled to collect?"
Why contractual adjustments matter most
Most reporting errors happen here. If contractual adjustments aren't mapped correctly, the metric becomes distorted. A practice may think collections are underperforming when the issue is bad adjustment logic. Or it may think collections are healthy because inappropriate write-offs are being mixed into categories that deserve closer review.
That means the formula isn't just arithmetic. It's a test of data discipline. Your practice management system, adjustment codes, payer setup, and posting rules all affect whether the number means anything.
A short explainer can help your team standardize the definition before you run monthly reviews:
Practical rule: If two managers in your organization define contractual adjustments differently, your net collection rate isn't reliable yet.
Before you compare one month to another, confirm that your reporting logic is consistent. The metric only works when the denominator reflects collectible revenue, not a mix of collectible and non-collectible amounts.
Calculating Net Collection Rate With a Real Example
A formula makes sense on paper. It becomes useful when you can run it against a clean set of numbers from an actual reporting period.
A simple practice example
Below is a basic example for a fictional medical group. The numbers are shown only to illustrate the math.
| Metric | Value | Notes |
|---|---|---|
| Total Charges | $500,000 | All charges billed during the period |
| Contractual Adjustments | $200,000 | Expected reductions based on payer contracts |
| Collectible Charges | $300,000 | Charges minus contractual adjustments |
| Payments Collected | $270,000 | Posted payer and patient payments |
| Net Collection Rate | 90% | Payments divided by collectible charges |
Start with total charges of $500,000.
Subtract contractual adjustments of $200,000. That leaves $300,000 in collectible charges. This is the amount the practice should be measuring itself against, not the original billed charges.
Then take payments collected, which are $270,000, and divide by $300,000.
The result is 90%.
How to read the result
The arithmetic is simple:
$270,000 / ($500,000 – $200,000) = 90%
What matters is the interpretation. A 90% net collection rate tells you the practice collected most, but not all, of the revenue it was entitled to collect after contractual reductions. It doesn't tell you why the missing portion wasn't collected. That's where operational review starts.
Look at the missing revenue as a set of questions, not just a shortfall:
- Were claims denied and never corrected
- Did patient balances age without follow-up
- Were underpayments posted without challenge
- Did staff write off balances that still had recovery value
This is also where reporting period discipline matters. If charges and payments are pulled from mismatched timeframes, the calculation can look better or worse than the actual operating performance. Keep the period logic consistent, and don't mix a lagging payment cycle with current-month production unless you're intentionally using a rolling method.
A good finance team doesn't just calculate the number. It reconciles the number to workflows, posting behavior, and payer performance. That's how a simple formula becomes a management tool instead of a dashboard decoration.
What Is a Good Net Collection Rate
The standard answer is easy. Public guidance commonly treats 95%+ as a strong benchmark for net collection rate, and it often presents NCR as the most accurate revenue-cycle KPI according to Benchmark Systems' discussion of net collection rate.
That benchmark is useful, but it's incomplete.
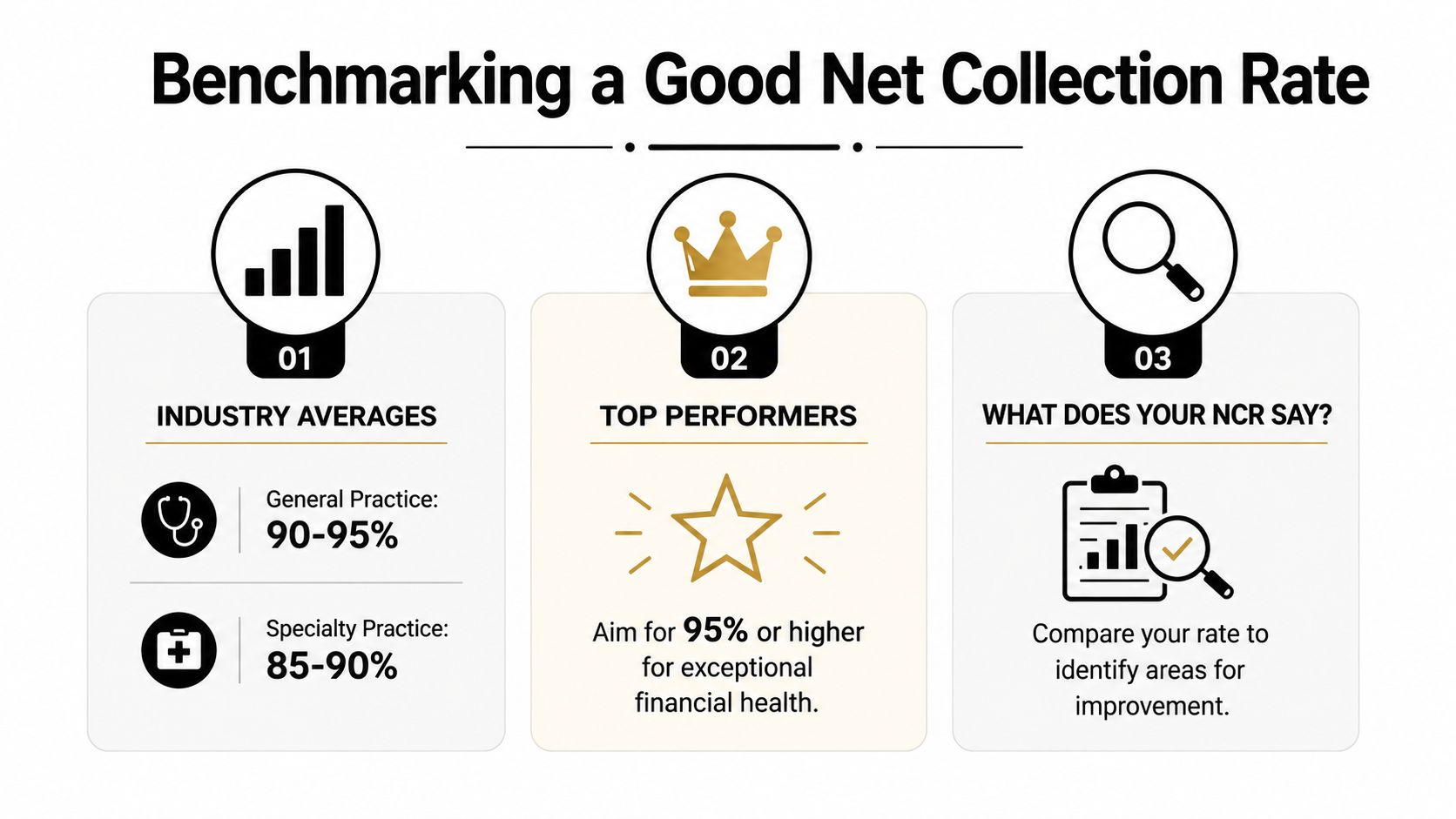
The benchmark answer
If your practice is below a strong benchmark, you probably have avoidable leakage. That's the straightforward case. Claims, balances, and follow-up activity deserve scrutiny.
If your practice is at or above that benchmark, many leaders stop investigating. That's where trouble starts. A high NCR can create false comfort if leadership assumes it automatically means the business is collecting well and protecting margin.
When a good number is a bad sign
A frequently underexplored question is whether a high net collection rate can still mask profit leakage if practices are aggressively writing off disputable balances or underpricing services. Public guidance commonly frames NCR as the most accurate revenue-cycle KPI and recommends 95%+ as a benchmark, yet it rarely explains how to reconcile NCR with underpayment appeals, fee-schedule drift, or service-line profitability using the same data set.
This is a real problem in multi-specialty groups and in organizations with high contract variance. Two practices can show the same net collection rate and have very different operating realities. One may be collecting appropriately against a disciplined fee schedule and strong denial management process. The other may be preserving NCR by accepting weak reimbursement, writing off balances too quickly, or failing to challenge underpayments.
A high net collection rate doesn't prove you're capturing full value. It may only prove you're collecting efficiently against a weakened baseline.
The context metrics that expose the truth
To judge whether a "good" NCR is actually good, pair it with a few surrounding measures and management questions.
Denied claim recovery
If denied claims are rarely appealed or corrected, your NCR may stay respectable while collectible dollars disappear before they ever become serious recovery efforts.Contractual allowance variance
If actual payer reimbursement drifts away from expected fee schedules and nobody monitors the gap, staff may post the difference and move on. NCR can still look healthy while contract performance deteriorates.Net patient revenue per encounter
If revenue per visit is softening without a clear mix or volume explanation, the issue may be pricing, payer reimbursement, or service-line economics rather than front-end collections alone.Aging trends and unresolved underpayments
If cash is erratic even with a strong NCR, inspect old balances, partial payments, and payer behavior. The metric may be missing friction that's occurring outside the way your reports are grouped.
A "good" net collection rate is good only when it aligns with the rest of the financial story. If margin is thinning, patient revenue per encounter is sliding, or underpayment work is weak, don't let one strong KPI override what your cash and income statement are already telling you.
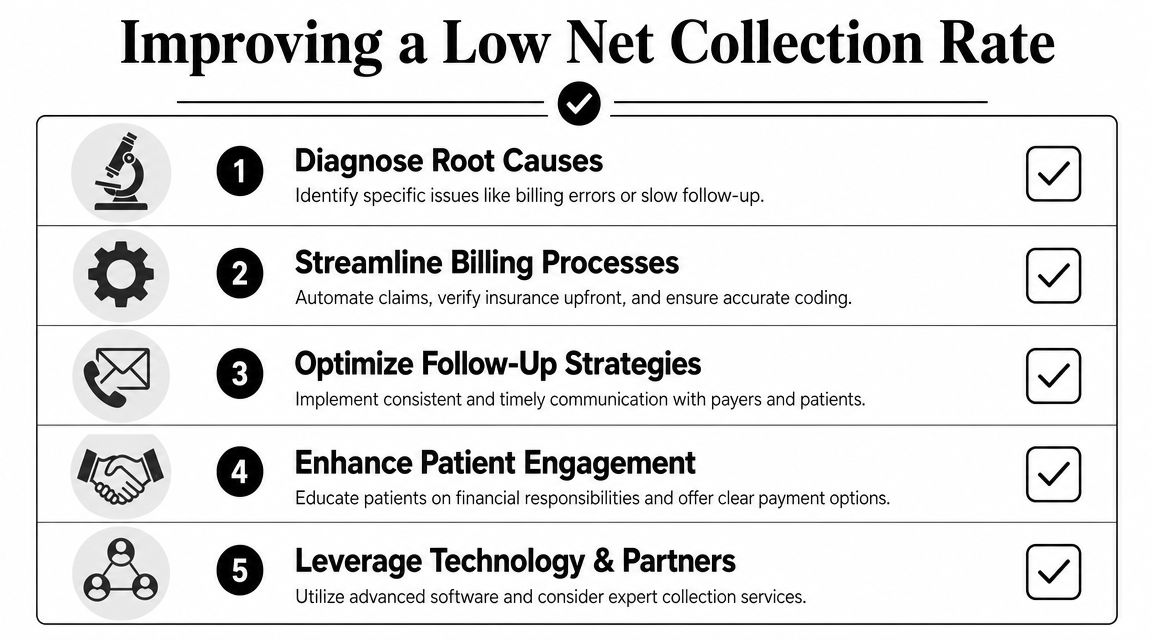
Diagnosing and Fixing a Low Net Collection Rate
When net collection rate is low, the fix usually isn't one heroic clean-up project. It's a chain of operational corrections. Revenue leakage enters at the front end, expands in the middle, and gets locked in at the back end if nobody owns the recovery process.
The fastest way to improve NCR is to audit the revenue cycle in sequence and force accountability by stage. A low number is rarely a mystery for long once you review eligibility, coding, claim quality, denial routing, and payment follow-up together.
Front end failures
The front end creates more downstream write-offs than most practices want to admit.
Eligibility isn't verified early enough
If coverage is checked late, or not rechecked when it should be, staff submit claims against the wrong plan, wrong dates, or inactive coverage. Fix this by tightening insurance verification before service, not after denial.Authorizations are handled inconsistently
When scheduling, clinical, and billing teams don't share ownership, authorizations fall through the cracks. Build a single work queue with clear status tracking and escalation rules.Patient responsibility is vague at check-in
If patients don't understand what they owe, balances shift into aging A/R instead of being collected while the encounter is still active. Use plain-language estimates, train front-desk staff on financial conversations, and offer immediate payment options.
Mid cycle breakdowns
Mid-cycle errors don't always create obvious denials. Sometimes they create delayed payment, underpayment, or avoidable rework.
Coding quality varies by provider or location
Review coding patterns by specialty, not just at the aggregate level. A single documentation habit can trigger repeated edits and recurring payer friction.Claims leave with preventable defects
Claim scrubbers help, but they don't replace disciplined charge entry and edit resolution. Staff need defined ownership for work queues and aging edits.Fee schedule maintenance is neglected
A stale fee schedule distorts expected reimbursement and weakens downstream analysis. In these situations, practices often benefit from targeted support, whether that's internal revenue integrity staff, software rules in the practice management system, or an outside group handling setup and oversight. One option some organizations use is claim adjudication and related RCM workflow support as part of a broader process review.
Low NCR usually reflects repeated small failures, not one catastrophic event.
Back end recovery problems
Collectible money is either recovered or surrendered.
A common issue is weak denial ownership. If nobody categorizes denials by root cause, staff spend all day touching claims without changing the pattern that created them. Build denial categories that matter operationally, then assign corrective actions to the team that caused the issue.
Another problem is passive follow-up. A/R staff may work oldest claims first without considering payer behavior, appeal deadlines, or underpayment value. That's activity, not strategy. Prioritize claims by recoverability and by the likelihood that delay will kill the balance.
Patient collections also need structure. Statements alone won't carry the load. Patients respond better when balances are explained clearly, digital payment paths are easy, and unresolved accounts are followed up with consistency.
A low net collection rate improves when leaders stop treating collections as a back-office clean-up task and start treating the entire revenue cycle as a controlled financial process.
Partnering with Clarity to Maximize Your Collections
Once a practice identifies where NCR is slipping, the next challenge is execution. Most organizations already know some of what needs to be fixed. They struggle because the fixes cut across scheduling, eligibility, coding, billing, posting, A/R follow-up, and reporting. Internal teams are often stretched thin, especially when they also have to support providers, patients, and operational leadership.
That is where an outside RCM partner can change the economics of the process. Not by chasing one metric in isolation, but by tightening the handoffs that determine whether earned revenue becomes posted cash.

What an outside partner should actually fix
A capable partner should address the operational points that distort or depress net collection rate:
Benefit verification before claims are at risk
Insurance Benefit Verification reduces avoidable eligibility problems before they become denials and rework.Fee schedule and system setup discipline
Fee Schedule & Practice Management Setup supports cleaner billing logic, better reimbursement expectations, and more reliable reporting.Claim status visibility and payment accuracy
Claim Status & Payment Posting helps the practice identify stuck claims, post accurately, and reconcile what payers did.Targeted support where staffing is thin
Billing Operations Support can cover specific functions instead of forcing a full outsourcing decision when the practice only needs help in selected areas.
How the operating model changes
The benefit isn't just more collection activity. It's better control. Leadership gets a clearer view of where revenue is slowing down, where staff are writing off too soon, and where payer behavior deserves escalation instead of acceptance.
That matters for forecasting. It matters for provider confidence. It matters for deciding whether a cash issue is caused by production, contract performance, front-end leakage, or unresolved back-end recovery. A strong operating model creates fewer surprises because the practice isn't waiting for month-end to discover what happened.
Clarity is one example of this model. As a full-service healthcare RCM partner, it handles services such as fee schedule setup, billing operations support, insurance benefit verification, and claim status with payment posting, which are the exact operational areas that influence whether net collection rate reflects real financial health or just surface-level reporting.
The best partnerships also preserve flexibility. Some practices need end-to-end support. Others need a narrow fix for denials, posting accuracy, or front-end verification. The right arrangement should match the actual leak, not force a larger scope than the business needs.
If your net collection rate looks acceptable but cash still feels inconsistent, or if the rate is plainly underperforming, the next step isn't another generic benchmark discussion. It's a working review of your current revenue cycle, your adjustment logic, your payer follow-up process, and the points where revenue is being surrendered.
If you want a practical review of where your collections process is leaking revenue, request a complimentary consultation with Clarity. The goal isn't to chase one vanity metric. It's to build a revenue cycle that supports cleaner cash flow, stronger margin, and fewer financial surprises.
Prepared with Outrank
No responses yet