You're probably looking at one of two problems right now. Your practice is busy, encounters are happening, providers are productive, and yet cash doesn't match effort. Or your team keeps calling denials “billing issues” when the underlying problem sits deeper in the payer decision process.
That gap is why practice leaders need to understand what claim adjudication is. Not as billing jargon. Not as a payer black box. As a financial control point that decides how much of your earned revenue becomes cash, how fast it arrives, and how much labor you burn chasing it.
If you run a practice, adjudication deserves the same attention you give staffing, scheduling, and reimbursement contracts. It determines whether a clinically valid service gets paid, reduced, pended, or denied. That's not clerical work. That's revenue governance.
Table of Contents
- The Hidden Engine Driving Your Practice's Revenue
- Defining Claim Adjudication for Financial Performance
- The Claim Adjudication Workflow Step by Step
- Decoding Claim Decisions and Common Denial Drivers
- Metrics That Reveal Your Adjudication Performance
- Improving Adjudication Outcomes with a Strategic Partner
The Hidden Engine Driving Your Practice's Revenue
Most month-end revenue surprises don't start with provider productivity. They start when payers apply rules to your claims.
A claim can represent appropriate care, solid documentation, and a legitimate patient need. None of that guarantees clean payment. The payer still runs the claim through eligibility checks, coverage rules, coding edits, timing rules, and policy logic before money moves. If your leadership team treats that process like back-office paperwork, you're leaving margin to chance.
The scale alone should reset how you think about it. A policy brief on real-time adjudication for health insurance claims estimates that adjudication-related expenses consume 3% to 6% of provider and payer revenues/premiums, translating to roughly $150 billion to $300 billion annually in the U.S. That's not a side process. It's one of healthcare's largest administrative cost centers.
Practical rule: If a process can delay payment, reduce allowed amounts, or trigger appeals, it belongs on the CFO's dashboard.
For physician groups and specialty practices, the takeaway is simple. Adjudication is where earned revenue gets converted into actual cash or gets trapped in rework. Your front desk influences it. Your coders influence it. Your clinical documentation influences it. But the financial consequence appears only after the payer makes its decision.
That's why strong practices stop asking, “Did we send the claim?” and start asking, “What decision did the payer make, why, and how quickly can we change the next outcome?”
Defining Claim Adjudication for Financial Performance

If you want the cleanest answer to what is claim adjudication, use this one: it's the payer's rules-based process for turning a submitted medical claim into a payment decision.
Consider a bank reviewing a loan application. The bank doesn't ask whether you'd like approval. It checks your information against a defined set of criteria. Health plans do the same thing with claims. They validate whether the patient was eligible, whether the service is covered, whether the diagnosis and procedure codes make sense together, whether authorization requirements were met, and whether the claim was filed on time.
What adjudication actually means
Operationally, adjudication is where a payer decides whether to pay the claim in full, reduce payment, pend it, or deny it. A practical explainer on the healthcare claims adjudication process describes it as the payer-side rule engine that validates coverage, coding, timing, and policy compliance, including checks for duplicate claims, member demographics, and diagnosis-to-procedure consistency.
Many practice leaders assume medically appropriate care should naturally lead to reimbursement. It doesn't. A claim can be clinically appropriate and still fail administrative logic. If eligibility is wrong, if authorization is missing, or if coding edits fire, the payer can deny or reduce payment anyway.
Here's the hard truth. Payers don't reimburse intent. They reimburse claims that satisfy contract and policy rules.
Rejection is not the same as adjudication
This is the distinction most articles miss, and it's one you should insist your team understands.
A claim rejection usually happens before true payer adjudication. It's often triggered by missing demographics, formatting problems, invalid subscriber data, or coding errors that stop the claim from moving forward. A claim adjudication happens after the payer accepts the claim into its decision workflow and applies benefit, policy, and payment logic.
A useful explanation from MedVision's overview of claim rejection and adjudication notes that many claims are stopped for basic errors like missing demographics or coding mistakes before they are ever adjudicated by the payer.
That distinction changes how you solve problems.
- If claims are rejected early, you fix front-end workflow. Registration quality, insurance capture, claim scrubbing, and coding edits are the priority.
- If claims are adjudicated and denied, you fix payer-facing issues. Medical necessity support, authorization management, contract interpretation, timely filing discipline, and appeal strategy matter more.
- If claims are adjudicated and reduced, you need payment variance review. The issue may be contract logic, bundling edits, or partial coverage.
Clean claim scrubbing prevents some losses. It does not replace adjudication management.
Leaders who blur rejection and adjudication usually assign the wrong team to the wrong problem. That's how denials repeat for months.
The Claim Adjudication Workflow Step by Step
Monday morning. Your dashboard shows a strong week of claim submissions, but cash is still lagging, A/R is aging, and staff are chasing payer responses. That gap exists inside adjudication. Once a claim reaches the payer, your revenue is no longer controlled by submission volume. It is controlled by how the payer applies edits, benefit rules, contract logic, and review queues to that claim.
What happens after submission
Claim scrubbing happens before the payer accepts the claim into its payment decision process. Adjudication starts after acceptance. That distinction matters because scrubbing catches obvious errors, while adjudication determines whether the claim becomes cash, a reduction, a denial, or a delay.
The first stop is intake. The payer system validates member status, plan enrollment, service dates, provider data, coding relationships, duplicate risk, and filing limits. Then it applies benefit and policy logic. Covered services, authorization requirements, diagnosis-to-procedure alignment, bundling rules, and payment methodology all come into play.
Straightforward claims often clear automated edits quickly. High-risk claims do not. They are pulled into exception handling, where payment slows and staff labor rises.
CMS explains in its partially adjudicated claims data resource that final Medicare claims processing can take weeks, while partially adjudicated claims can reach ACO REACH participants 2–4 days after providers submit claims, with updates delivered daily.
That matters for practice leadership. Adjudication is not always one final yes-or-no event. It often unfolds in stages, with status changes that affect expected cash timing, follow-up priorities, and forecast accuracy.
A short video overview helps make that sequence easier to visualize.
Where claims slow down
The main choke point is the pend queue.
A pended claim is not harmless. It ties up expected revenue, extends days in A/R, and creates rework for billing, coding, and front-desk teams. If you only monitor submission counts, you miss the financial risk building inside these queues.
Manual review usually starts when the payer sees missing support, conflicting data, coordination of benefits issues, policy-sensitive services, or exceptions that do not fit automated rules. These claims cost more to collect because they require touches. Every extra touch reduces margin.
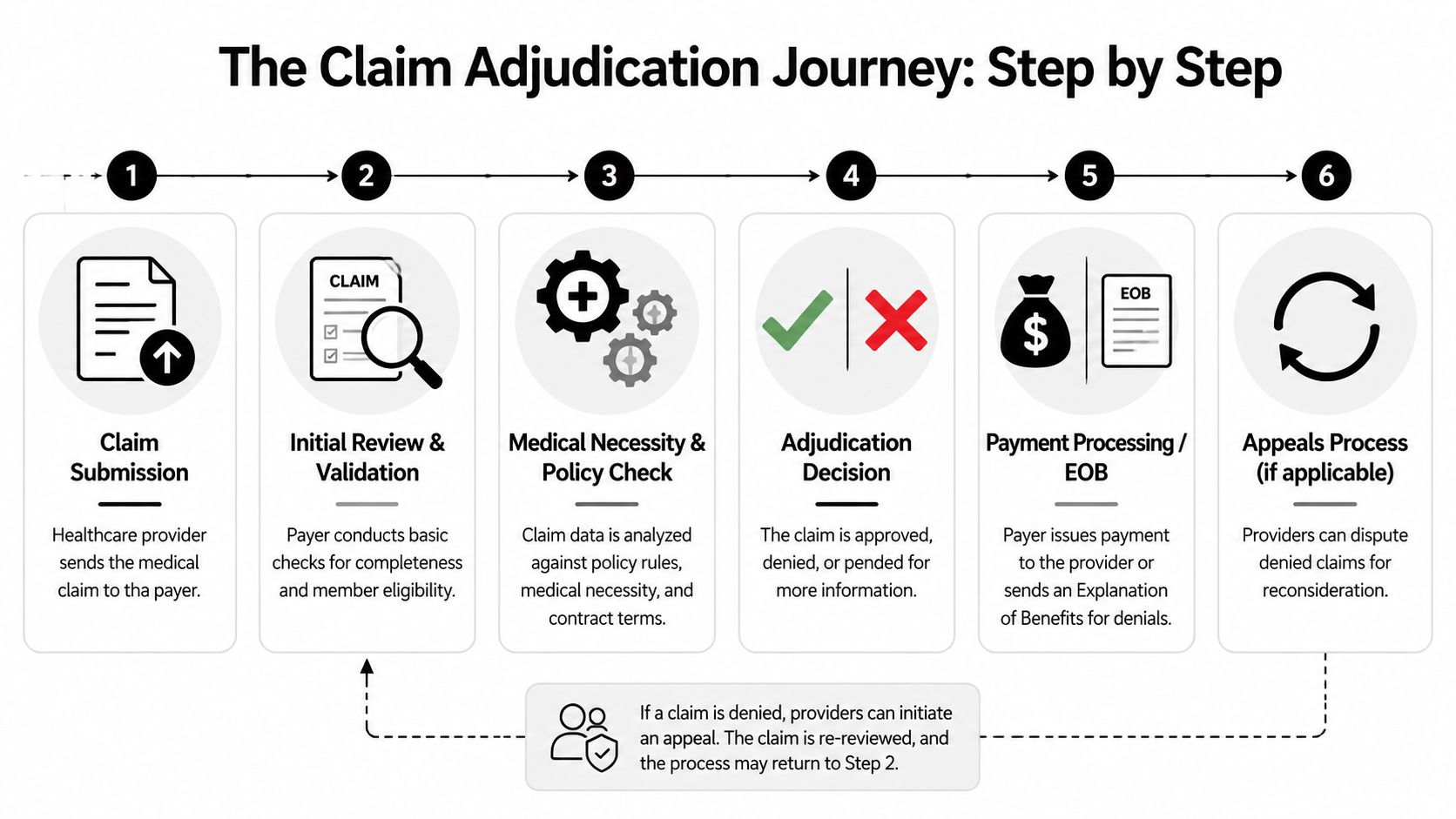
Use this workflow as your management view:
- The payer accepts the claim and runs intake validation.
- Automated edits review the claim against eligibility, benefits, coding rules, duplicate logic, and filing deadlines.
- Payment logic is applied to allowed amounts, contractual rules, and patient responsibility.
- Exception claims pend for manual review, documentation requests, or additional investigation.
- The payer issues a decision with payment, reduction, denial, or pend status details.
- Your team acts on the result through posting, variance review, correction, resubmission, or appeal.
Submission is an activity metric. Adjudication is a financial control point.
If you run a practice, manage this workflow like cash management, not clerical processing. Teams that treat adjudication as back-office paperwork usually find problems late, appeal too much, and collect too slowly.
Decoding Claim Decisions and Common Denial Drivers
The remittance is not paperwork. It is the payer telling you exactly how much cash you earned, how much was held back, and how much work your staff just inherited.
That distinction matters because many practice leaders confuse front-end claim scrubbing with adjudication. Scrubbing tries to stop obvious errors before submission. Adjudication is the payer's financial decision engine after the claim arrives. It applies coverage rules, contract terms, medical policy, coding edits, and patient liability logic. If you treat that outcome as routine billing output, you will miss where margin is leaking.
The four core outcomes
Every adjudicated claim lands in one of four buckets:
- Paid in full. The payer accepted the claim and reimbursed as expected under the contract and benefit plan.
- Partially paid or reduced. The claim was payable, but the payer cut part of the charge based on fee schedule limits, bundling logic, non-covered components, or patient responsibility.
- Denied. The payer refused payment and assigned the account back to your team for correction, appeal, adjustment, or write-off review.
- Pended. The claim is still unresolved because the payer needs records, manual review, coordination details, or another exception check.
A paid claim posts cash. Every other outcome creates friction. Reduced claims need variance review. Denied claims need labor. Pended claims trap revenue in limbo and usually come back with more staff touches attached.
Where denial management goes wrong
The mistake is treating all denials as administrative noise. They are not. They are signals.
A denial tells you where one of four controls broke down: registration, coding, documentation, or payer rule management. If your team only works denials one account at a time, you recover some dollars but fail to fix the source of the problem. The result is predictable. The same denial repeats, rework grows, and net collection erodes.
Use denial categories to find the broken control, then fix that control upstream.
Common denial reasons and first-step fixes
Use this table to decide what action protects cash fastest.
| Denial Reason / Code Category | What It Means for Your Practice | First Action to Take |
|---|---|---|
| Service not covered | The plan excludes the service, the benefit limit was met, or the service was billed under the wrong benefit structure | Confirm the benefit terms, then shift the balance correctly to patient responsibility, rebill if the service was misclassified, or adjust if no recovery path exists |
| Incorrect patient information | Demographics, subscriber data, or member ID did not match payer records | Audit registration accuracy, correct the account, verify eligibility, and resubmit quickly before aging increases |
| Diagnosis and procedure mismatch | The claim did not support medical necessity or code pairing under payer edits | Review coding against the chart, correct code selection if needed, and submit documentation only if it directly supports payment |
| Timely filing issue | The payer says the claim or corrected claim missed the filing deadline | Pull submission history, clearinghouse acceptance records, and proof of receipt, then appeal only if you can document timely filing |
| Authorization missing or invalid | The payer could not match the service to an approved authorization | Validate the authorization number, dates, units, and servicing provider, then correct the claim or escalate for appeal if the approval exists |
| Medical necessity denial | Clinical records did not meet the payer's policy standard for the billed service | Compare documentation to the payer policy, then decide quickly whether the record supports an appeal or whether staff time should be preserved for stronger recoveries |
The first move matters. A registration denial usually needs correction and resubmission. A medical necessity denial needs policy review before anyone starts an appeal. A contract underpayment issue belongs in variance analysis, not in a generic denial queue.
That is how strong RCM teams protect margin. They do not chase every denial with the same playbook. They sort by recoverability, dollar value, filing deadline risk, and payer pattern. High-probability recoveries move first. Low-value, weak-documentation accounts do not get unlimited labor.
Run this process like financial triage. Adjudication decisions determine cash timing, write-off exposure, and staff cost per claim. If your denial strategy does not reflect that, the payer is controlling your revenue more tightly than you are.
Metrics That Reveal Your Adjudication Performance
If you can't measure adjudication performance, you can't control it. Most practices track charges and collections. Fewer track the indicators that explain why collections lag.
The dashboard that matters
Start with a compact scorecard.
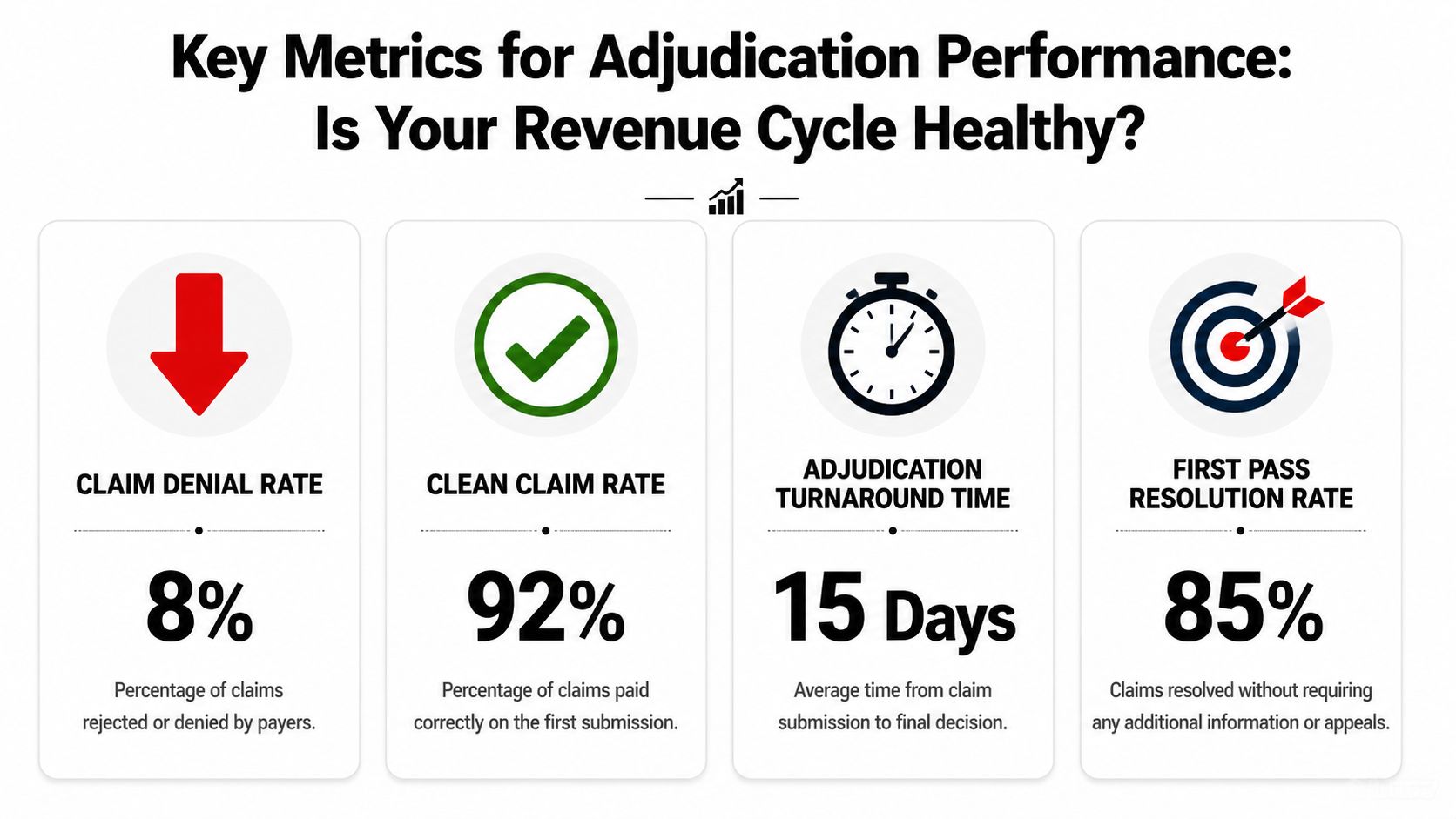
- First pass resolution rate tells you how many claims resolve without rework. If it's weak, your upstream processes or payer-specific rules are breaking down.
- Denial rate shows how often payers reject payment after adjudication. This is one of the clearest signals of preventable friction.
- Days in A/R tells you how long revenue is sitting unpaid. Adjudication delays, poor follow-up, and appeals backlog all show up here.
- Pend volume by payer and reason helps you spot where automation stops and manual intervention starts.
These metrics matter because adjudication is high-volume and mixed in complexity. As noted earlier, a policy brief estimates that U.S. insurers adjudicate over 3 billion medical claims each year, and while about 80% are processed automatically, the remaining 20% require manual review and represent the most complex, high-risk claims. That manual segment directly affects denial rates and days in A/R.
What weak metrics usually mean
Poor numbers rarely come from one department.
A rising denial rate usually points to front-end eligibility errors, weak authorization discipline, coding mismatches, or payer rule changes that nobody operationalized fast enough. Higher days in A/R often mean your team is posting correctly but not escalating pended and denied claims with urgency.
Use a simple management lens:
| Metric | What a weak result usually suggests |
|---|---|
| First pass resolution rate | Bad registration data, weak coding edits, inconsistent claim preparation |
| Denial rate | Repeatable workflow errors, payer-specific rules ignored, documentation gaps |
| Days in A/R | Slow follow-up, appeal delays, unresolved pends, payment variance not reviewed |
| Pend volume | Claims are hitting complexity triggers that your current process isn't preventing |
Watch trends by payer, specialty, and denial category. Aggregate numbers can hide the real problem.
Don’t chase vanity metrics. Track the indicators that tell you whether claims convert to cash cleanly and predictably.
Improving Adjudication Outcomes with a Strategic Partner
Monday looks strong. The schedule is full, charges go out on time, and the billing team says claims were scrubbed and submitted cleanly. Three weeks later, cash is short, pends are piling up, and denials are rising by payer. That is not a clerical miss. It is a failed financial control.
Claim scrubbing helps you catch missing fields, invalid codes, and basic formatting problems before submission. Adjudication is different. It is the payer’s payment decision, based on benefits, edits, medical policy, authorization status, documentation support, and contract terms. Practices that confuse the two usually overestimate how much control they have after a clean claim leaves the door.
If you want better adjudication outcomes, fix the inputs that drive payer decisions and tighten the follow-up process that protects cash after submission.
The operational fixes worth making now
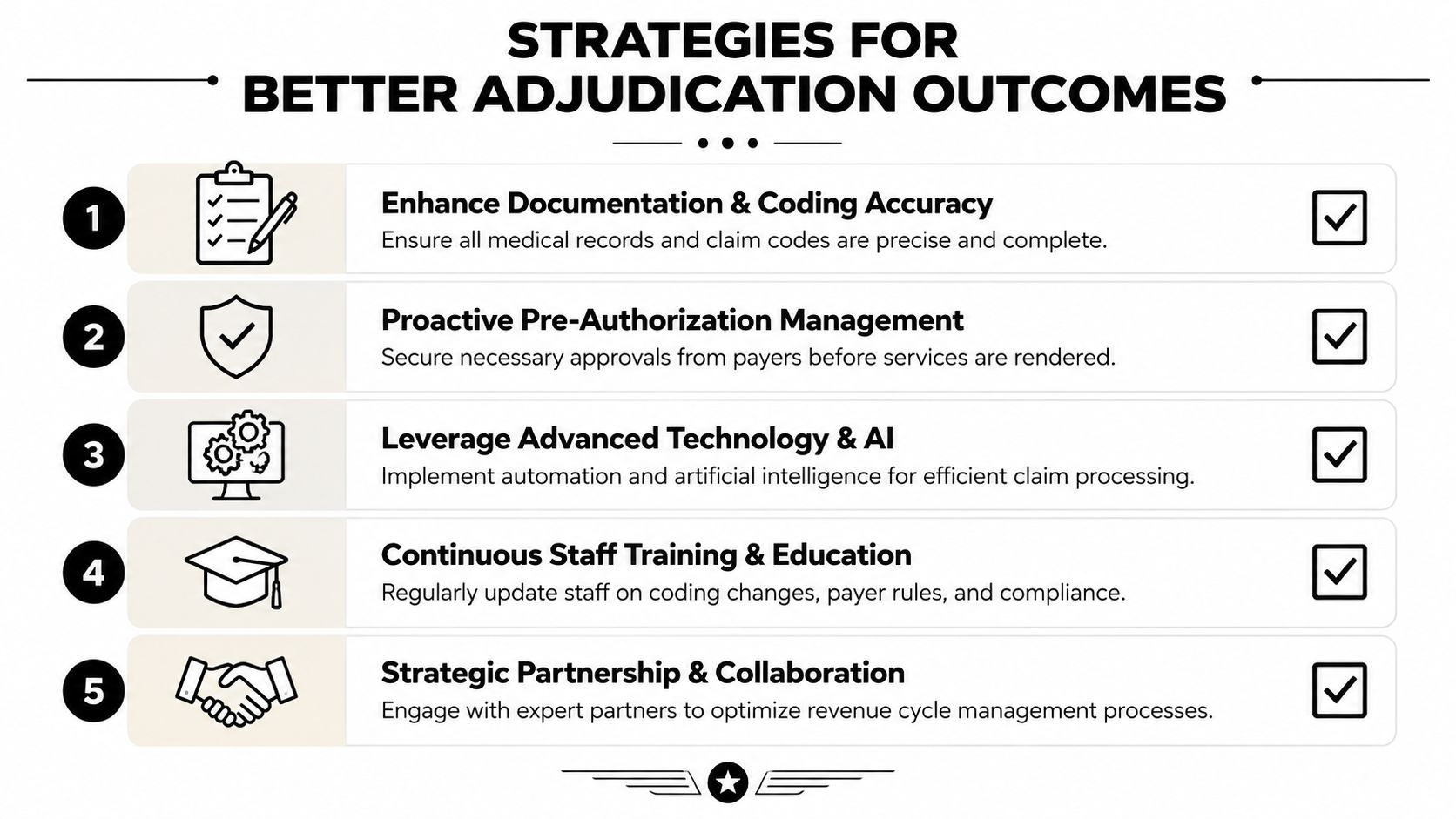
Start with the breakdowns that cost money fastest.
- Tighten insurance verification: Confirm active coverage, plan rules, coordination of benefits, and patient responsibility before the visit. Bad eligibility data creates avoidable denials and rework long before the payer adjudicates the claim.
- Put one owner over authorization discipline: Required approvals should never sit between scheduling, clinical staff, and billing with no accountability. Build payer and service-specific rules into the workflow and track them daily.
- Audit coding against documentation routinely: Many adjudication failures start with records that do not support the billed level, diagnosis linkage, or modifier use clearly enough for payer review.
- Use claim scrubbing for what it does well: Scrubbers catch technical defects. They do not manage payer policy, contract interpretation, or medical necessity logic. Treat them as a gate, not a strategy.
- Create denial-specific work queues: Separate simple corrections from appeals, underpayments, and pended claims that need escalation. Different problems need different staff time.
- Review payment variances aggressively: Partial payment is still a revenue leak. If allowed amounts, bundling, or reductions are not reviewed, your practice absorbs losses it never approved.
Ownership matters as much as process. Front desk and eligibility teams prevent bad data from entering the claim. Coders and charge capture staff make sure the billed service matches the record. Billing staff submit accurately and flag exceptions early. A/R follow-up teams work pends, denials, and underpayments by dollar value, aging, and likelihood of recovery. Leadership reviews payer patterns and forces operational changes when the same issue shows up twice.
The goal is not to process denials faster. The goal is to stop producing avoidable denials and recover the rest with discipline.
When outside support makes financial sense
Internal teams hit a ceiling. You see it when supervisors spend their week clearing edit queues, answering posting questions, chasing payer responses, and reviewing appeals that should have been prevented upstream. At that point, senior labor is being used to hold together an unstable process.
In these situations, an external RCM partner can make sense. The value is not just extra hands. It is tighter execution across verification, claim submission, follow-up, posting, and denial recovery, with clearer accountability for results.
Clarity provides full-service healthcare revenue cycle management, including insurance benefit verification, billing operations support, claim status follow-up, and payment posting. That type of support fits practices that need full-cycle management or targeted help in the parts of the workflow that have the biggest impact on adjudication results.
Use a partner when you need one or more of these:
- Specialized follow-up capacity: Your team gets claims out but cannot keep up with pends, denials, and underpayments.
- Process redesign: You know the losses are systematic, but nobody internally has the time to rebuild the workflow.
- Coverage gaps: Growth, turnover, or leave has created weak points in verification, billing, or posting.
- Leadership visibility: You need cleaner reporting on where claims stall, which payers create friction, and which issues are draining margin.
Do not outsource chaos. Define the outcome first, then decide who should execute it. Lower preventable denial volume. Faster pend resolution. Cleaner posting. Better variance recovery. Tighter payer accountability.
Treat adjudication like the financial control point it is, and your operating priorities get clearer fast. Strengthen the data before submission, enforce documentation standards, separate scrubbing from true adjudication management, and assign real ownership to follow-up. That is how practices protect margin instead of explaining it away.
6 Responses
[…] handoff between claim submission and payer decision also matters. Teams that understand claim adjudication in healthcare usually recover faster because they know where a claim can stall, reject, pend, or short-pay before […]
[…] and they help finance model what is likely to happen next. If a payer starts adding friction during claim adjudication and payment review, the point is not just to count denials. The point is to forecast the cash impact, adjust follow-up […]
[…] reviewed. For readers who want a plain-English explanation of that review process, this overview of claim adjudication for CFOs and CEOs explains how insurers decide what they will […]
[…] leaders who want a plain-language view of that process, this guide on what claim adjudication means in practice is a useful […]
[…] The claim is generated and submitted. After that, the payer adjudicates it. If you want a plain-language overview of that payer decision step, see this explanation of claim adjudication. […]
[…] your team wants a better grasp of where those edits happen in the payment process, this overview of claim adjudication in healthcare billing is a useful […]